Get the latest on metabolic psychiatry. Subscribe.

Listen, Watch & Subscribe on:



Metabolic Therapies for Psychiatry: State of the Evidence
Listen
About the host

About the guest

About the guest

About the host
About the guest
About the guest

Bret:
Welcome to the Metabolic Mind Podcast. I’m your host, Dr. Bret Scher. Metabolic Mind is a nonprofit initiative of Baszucki Group where we’re providing information about the intersection of metabolic health and mental health and metabolic therapies, such as nutritional ketosis as therapies for mental illness.
Thank you for joining us. Although our podcast is for informational purposes only and we aren’t giving medical advice, we hope you will learn from our content and it will help facilitate discussions with your healthcare providers to see if you could benefit from exploring the connection between metabolic and mental health.
Welcome to Metabolic Mind, a nonprofit initiative of Baszucki Group, where we explore the evidence and experience connecting metabolic and mental health.
And metabolic therapies like nutritional ketosis as a treatment for mental illness. But how strong is the evidence supporting nutritional ketosis or a ketogenic diet for treating conditions ,such as depression or bipolar disorder, schizophrenia, or even anxiety, PTSD, OCD, and other symptoms? It all depends on how you interpret the question of how strong is the science?
So, in this video, I interviewed two physician scientists, who know and contribute to the scientific research and also experience the daily caring for patients with mental illness. Stanford psychiatrist and founder of the Stanford Metabolic Psychiatry Clinic, Dr. Shebani Sethi.
And Dalhousie, I always mispronounce that, Dalhousie psychiatrist and researcher, Dr. Cynthia Calkin, whose TRIO-BD Study was awarded the 2023 Paul Wender Best Paper in the Journal of Clinical Psychiatry Award. And as you’ll hear, the combination of knowing the science, the neural mechanisms, and the strength of the evidence can sometimes be at odds with knowing what to do with the patient right in front of you.
And that’s the perspective that these physician scientists bring that I think is so valuable. So, we start the interview discussing the science. But the key takeaway messages come later when we discuss how to differentially interpret the strength of the science depending on whether you’re a loved one of someone living with serious mental illness or if you’re a treating psychiatrist or someone writing treatment guidelines, right?
Because each situation requires a different level of scientific certainty. So, keep listening to get those important caveats. But before we get into the interviews, please remember our channels for informational purposes only. We’re not providing individual or group medical or healthcare advice or establishing a provider patient relationship.
Many of the interventions we discuss can have dramatic or potentially dangerous effects if done without proper supervision. Consult your healthcare provider before changing your lifestyle or your medications. Now first, let’s hear from Dr. Sethi and what she thinks when someone says there isn’t enough scientific evidence to support treating serious mental illness with nutritional ketosis.
Shebani:
The short answer to that is we don’t have a lot of evidence for ketogenic diets, specifically in mental health. But there is a growing interest in it because of past research that has been done in the field of neurology. We’ve been using ketogenic therapies in the field of neurology for about a hundred years and to treat pediatric epilepsy.
So, we know that ketogenic therapies are helpful for seizures. And there’s a lot of basic science research and data, both preclinical and clinical, that have been focused on how ketogenic diets can improve brain health. So, one of the things that metabolic psychiatry is focused on is how metabolic dysfunction can be targeted to improve both metabolic and mitochondrial health.
How our current therapies are targeted to basically improve pathways that are responsible for energy and cellular metabolism. So, we really want to look at how best we can determine the contributions of these metabolic dysfunctions to neuronal energy deficits, and the significant changes in brain structure and function that do occur post these interventions.
And that’s what we are looking at today with ketogenic diets, specifically in brain health.
Bret:
So, part of the scientific understanding is connecting underlying potential mechanisms for how metabolic therapies, like nutritional ketosis, can impact brain function and symptoms of mental illness. Dr. Sethi co-authored a paper with Dr. Judy Ford exploring these mechanisms, one of which was a more efficient fuel source for the brain.
So, let’s hear how Dr. Sethi explains what we know about more efficient fuel than some of the other mechanisms.
Shebani:
So, we can look at ketones, and we can measure Gibbs free energy. You have about almost 30% more energy from ketones than you do from glucose when the brain is burning ketones versus glucose.
So that’s one example. But nutritional research, in general, has acknowledged that diet does affect several processes in the brain, which include biological processes, like mitochondrial activity and function, immune function, inflammatory function, oxidative stress, and monoamine activity. So, I’m talking about neurotransmitters, serotonin, dopamine, and essentially, a ketogenic diet provides this alternative fuel.
It circumvents kind of the main system that we typically use when we burn glucose, to generate ATP and energy. And what’s interesting to note is that we know that ketogenic diets have been helpful for epilepsy and for brain health, and we know some of the mechanisms behind that. Of course, there’s more to learn, but in mental illness almost a hundred years ago, some of the oldest biomarkers in psychiatry that were discovered included lactate.
So there were increased lactate levels and there were lower, glutathione levels. And these are markers that indicate to us that there’s bioenergetic dysfunction. So we’re seeing more evidence of a dysregulated metabolism in the pathophysiology of major psychiatric illnesses like schizophrenia.
Bipolar illness as well as major depressive disorder. So there’s really a problem with handling glucose in the brain and insulin resistance and changes in glucose metabolism. actually proceed the onset of psychiatric disease. So we have meta-analyses that tell us and demonstrate that there’s an abnormal glucose and insulin signaling present in patients that have been diagnosed with their first episode of psychosis and have not started medication yet.
So, that’s a really important thing to realize is that there’s something happening beforehand, which is a different emphasis from the past. There’s also insulin resistance that’s been identified as a risk factor for major depressive disorder. And some of the work that Bruce McEwen and Bob Sapolsky have done in the past looked at stress and cortisol, and how that’s neurotoxic to the brain, specifically the prefrontal cortex as well as the hippocampus, which is very important for memory formations.
And if glucocorticoids are affecting our neurons this much, and we’re learning from their work also that insulin resistance is part of that mechanism, then why aren’t we focused more on targeting that insulin resistance? We know that ketogenic metabolic therapies are very effective for improving insulin resistance.
We know that certain ketones, like beta hydroxybutyrate, there were some studies looking at how ketones specifically actually, if you looked, in animal studies, if you looked at slices of the hippocampus, there was more resistance to stress with ketone exposure, and that was compared to controls.
So, there’s a lot of interesting ways to look at why ketones would be helpful for illnesses, such as mental illness like schizophrenia or bipolar illness.
Bret:
is it enough to know that metabolic dysfunction precedes psychiatric diagnoses? Is it sufficient to understand that nutritional ketosis can improve metabolic dysfunction?
Are those quote unquote enough to change clinical care? Again, here’s Dr. Sethi.
Shebani:
I think we have good evidence that shows beneficial effects on metabolic health, like improving blood glucose, insulin resistance, triglycerides, cholesterol, et cetera. But with mental health specifically, the evidence needs to be at a more robust level in order for it to actually be part of standard care or clinical practice guidelines.
I do use ketogenic therapies in mental health. And I study it, research it as well, as many other people do. So, if we think about the current state of evidence, the current state of evidence has really right now, case series, case reports, expert opinions, some observational studies, retrospective data.
We did a pilot at Stanford looking at ketogenic diet in schizophrenia and bipolar illness. It was a pilot of 24 patients. And it’s a pilot study so it wasn’t randomized. And that’s the first step before you go to randomized trials. There’s another group working on a pilot in the UK also looking at schizophrenia and bipolar illness, along with looking at cognitive outcomes, looking at metabolomic data as well and imaging.
There are two randomized control trials underway currently. One at UCSF, and one in Australia. And the one at UCSF is focused also on brain imaging, functional connectivity, looking at cognitive outcomes as primary, so functional connectivity and cognition as primary outcomes. So ,there are trials underway, and I’m talking about with the major illnesses, like schizophrenia, bipolar illness and depression as well.
There’s also a randomized control trial that’s also being planned and started and recruiting this year as well just with depression alone and college mental health population with eating disorders and other illnesses. There’s also case series and case reports and observational data and retrospective data.
So, it’s a gradual process of starting with these kinds of studies before you get to increase amounts of funding is needed to do randomized control trials. And also ethically, you have to follow that progression so that you’re planning a randomized control trial in the right manner.
So, with eating disorders, there’s been some improvements also with metabolic health as well as binge and purge episodes, and that’s been documented in the literature. So, that’s really interesting, too, from a dietary perspective going on a diet, and how that’s actually improving since typically we don’t want people to be dieting when they have an eating disorder.
However, ketogenic metabolic therapy is a bit different, different bird.
Bret:
No, I think that’s a fantastic point. Dr. Sethi talks about ketogenic metabolic therapy, not a standard keto weight loss diet. You may wonder what the difference is, and it can be subtle in some cases. But the idea is to ensure the patient is in, and remains in, ketosis, possibly trying to achieve specific blood or breath ketone levels.
The goal isn’t weight loss. The goal is achieving ketosis and maintaining it. So, now let’s hear from Dr. Cindy Calkin about how she would sum up the state of the evidence connecting metabolic and mental health and metabolic therapies as treatment for mental illness?
Cynthia:
In terms of evidence, the TRIO-BD Study is a quadruple mast placebo control trial.
So, gold standard evidence. it’s a smaller trial. We had a sample size of 45. Some of that was due to COVID, which made us stop the study short. But we had very large effect sizes, and it was hypothesis driven. So, I think that we can trust that evidence. Our statistician told us that we could trust the evidence based on it being hypothesis driven in the large effect sizes.
I think we need, that needs to be replicated. I think we need to look at more mechanisms. I think that insulin resistance is related to bipolar disorder, I think through a common pathophysiology. There’s very complex metabolic pathways where psychiatric illness fits in there, and and I think one kind of plays on the other.
And so it makes sense to me, that metabolic dysregulation is part of psychiatric illness. And for me, because I see and treat patients with bipolar disorder, that I’m quite certain that it’s part of a bipolar disorder based on some of these other cortisol studies and things like this.
There’s also been work done by, Ana Andreazza, looking at mitochondrial dysfunction and oxidative stress and whatnot. And she’s looked at inflammatory markers early in the course of bipolar disorder. And later on, we had done a hypothesis paper looking at how bipolar disorder tends to progress. And it’s usually later in the course of bipolar disorder that this metabolic dysregulation really starts to impact the bipolar disorder and change or modify the course of illness to a neuroprogressive treatment-resistant, chronic form of illness.
So, that’s my understanding of, of how they fit together and sort of state of things. A lot of it is at each of these sort of stages of the metabolic pathway, we could intervene with the hypercortisolemia. There are drugs that will lower cortisol. Whether that works, whether that’s what we should do, I don’t know.
Maybe mindfulness meditation might be a way to bring down cortisol levels? Like there could be all sorts of different approaches that could help at each of these stages. Anti-inflammatory immune, modulators, like all of these things, things that would, superoxide dismutase would be something that might work on oxidative stress.
So there’s all these different things, which is really exciting for me, and none of them are psychiatric drugs.
Bret:
Now, Dr. Calkin mentioned her TRIO-BD paper, which is paradigm shifting work. The study demonstrated that treating metabolic disorders improved psychiatric symptoms. We have a longer podcast where we go into the study in much more detail. So, if you’re interested, I encourage you to listen there because it’s really a fascinating study that deserves more attention.
But next, I ask Dr. Sethi to tell us about the pilot study she ran, and how it fits into the context of other ongoing or completed studies. This will help us get a better idea of the current state of the evidence.
Shebani:
Yes, not all the data has been analyzed yet. But we will be presenting that data at the International Conference for Bipolar Disorders in Chicago, in June, this year.
We have analyzed half the cohort so far, and we did see a 25% reduction in depression, 39% reduction in anxiety, measured by GAD-7 and PHQ-9. With depression, we saw a 33% change in the clinical global impression scale, and 23% improvement in quality of life. As well as about 30% improvement in sleep.
If we looked at metabolic markers, we saw 17% reduction in inflammatory markers, specifically improvements in HDL by 8%, 21% improvement in triglycerides set translates down to a 39 point reduction, which can be significant for people. Visceral fat, we also looked at, and there was a 31% reduction, a 19% reduction in fat mass alone, and 11% weight reduction with no drug.
So, that is over a four month period of intervention itself. So, it’s encouraging results, and it’s definitely worth studying further.
Bret:
It’s certainly encouraging to hear about the beneficial metabolic results Dr. Sethi saw in her study. But here’s an important question. If we were to use a drug to induce weight loss, do you think we would see the same metabolic and mental health benefits?
Shebani:
The ketogenic diet has a lot of, because you’re really focusing on improving metabolic parameters in multiple areas, whereas some of the medications only specifically work mechanistically on maybe one, potentially two, areas. And since the ketogenic therapy is really more system wide, I think you end up seeing more benefits in that respect.
And of course, we don’t have data like comparing the two interventions, but they certainly, at least clinically, I see that there is a place for medications that can be helpful for some people. But certainly, if there’s a nutritional intervention or metabolic intervention that has less side effects ,like a ketogenic diet, it’s a very different, it’s a different feeling for people who are struggling through this illness and much more favorable.
Bret:
That’s such a great point. Nutritional ketosis can have fewer side effects, or even beneficial external effects, compared to medications. But how did Dr. Sethi’s study participants do with the keto diet? Were they able to safely and effectively implement it? And were there any concerning side effects?
Shebani:
Yeah, I have found it to be safe and well tolerated, too.
It is important, especially when patients are on medications, other medications, whether they’re psychiatric or not, it’s really important to be monitored and to be seeing a physician, ideally, who’s familiar with this. That’s really important. And so that makes the safety all the more better and the more tolerable, too.
And being able to proceed, especially initially during the keto adaptation period, knowing what side effects maybe to expect when you’re changing from your previous diet. For example, a standard American diet where there’s a lot more carbohydrates and sugar compared to a ketogenic diet, which has a lot less.
And you’re typically increasing fat content as well compared to what you were having before. It’s important that your body needs time to adjust and also to understand that difference and what to expect. Going to somebody that knows what they’re doing is really important.
Bret:
Now, next, we explore the concept of balancing the need for evidence versus caring for the patient in front of you.
First, let’s hear from Dr. Calkin.
Cynthia:
I think based on our outcomes study and based on the TRIO-BD clinical trial, that we have evidence to look for and treat insulin resistance if it’s present. And based on that, we have the underlying mechanism that’s worsening the course of bipolar disorder.
And we know metformin only works 50% of the time. So, I start with metformin. When they’re well enough, we add diet and exercise. If that doesn’t work and they’re still insulin resistant, I start looking at other insulin sensitizing medications and other ways of sensitizing patients to insulin in a lot of ways.
When you’ve come to the end of the line and someone has been sick for 25 years and failed all classes of psychotropic medications, you have to start looking elsewhere. But I think it’s really important that you have to have a rationale. You have to have an understanding of the underlying mechanisms, and it has to make sense.
So, we can’t just start pulling things out of the air. Let’s try this, let’s try. There has to be, you have to think through what are the potential pathways. And that’s what I did with my first hypothesis paper was how do these things overlap? And I did a paper, in 2012, and here’s how long it takes for things to catch on. Type II diabetes and bipolar disorder are more than just comorbid disorders.
That has now had more than 6,000 reads, but it’s 10 years later, And it took a good five or six years before people really started reading it, and it was published in the Annals of Medicine because psychiatry wouldn’t touch it. And I’ve published Annals of Medicine a number of times, when psychiatry, but really, I need it to be in the psychiatry literature.
Because as psychiatrists, we need to be really looking at it.
Bret:
And here’s a similar question for Dr. Sethi. How do we see the evidence differently if we’re writing clinical guidelines or if we’re treating psychiatrists, or if we are a loved one of someone living with serious mental illness?
Shebani:
I would be very transparent with them about what is the evidence that we have today and what evidence that we are working on for the future, where that comes into play for changing practice or guidelines. And I would tell them what I’ve seen clinically that’s been helpful, what potential side effects they may expect.
And generally ,with a nutritional approach, people are not as concerned about side effects, right? So there’s a little bit more, I guess, there’s less barriers to trying. And I think that’s helpful for people to know. It’s also important that they’re frequently monitored, and I think they feel more comfortable with that. There isn’t harm in. In doing a ketogenic diet intervention with a patient, unless you’re maybe not experienced or skilled in that area, or you don’t necessarily know how it interacts with medications. That’s a different story.
So, I think it’s important that whoever the family member is, where they go and who they’re going to is really important. It becomes an important quality and safety piece.
Bret:
And a common question we hear often is, can I stop all my medications when I start a keto diet? The answer is definitely not. We would never recommend anyone suddenly stop psychotropic medications.
Many people may be able to taper slowly after they’re stable on the diet. But this requires medical supervision from your prescribing clinician and is very individualized to each person. Now, we do hear encouraging anecdotal reports of some people being able to reduce medications over time, and in some cases, to even eliminate them.
And we have a whole video specifically on this topic, but let’s get Dr. Shebani Sethi’s point on this.
Shebani:
Yeah, I worry about that line of thinking because getting off a medication is a big deal. And no matter what, there really should be frequent communication and collaboration with their doctor. If they want to try a ketogenic metabolic therapy and they’ve identified someone that they want to work with, the doctor should definitely be involved in that conversation as well as, being aware of it and also monitoring medications.
Ideally, it’d be great if there was a doctor that does all that together. But for some people, that’s not the case. And there may be a nutritionist who’s an expert in a ketogenic therapy and might be able to provide that piece, but the psychiatrist or the primary care doctor or the doctor that they choose to work with needs to also be aware of what’s going on. And that’s really important, too.
Bret:
Okay, so now let’s shift to the treating physician, the clinician who’s accustomed to waiting for the randomized controlled trial to get published in the New England Journal of Medicine before changing their clinical practice.
Because that’s what happens with medications, right? So, should they hold the same standard for nutritional ketosis, or should they apply a different set of parameters to a nutritional intervention?
Shebani:
Yeah, I think that’s a really interesting question because we’ve already seen in the nutritional psychiatry research world, that Mediterranean diet, for example, has been helpful with depression.
And that was a randomized control trial. But how much of psychiatry actually adopted that as part of standard practice? That’s questionable. I don’t know the numbers, but I don’t think it’s very high. So, how much exercise, physical movement, which we know is very good for cognition, especially for in mental health, also, how much of that is emphasized?
How much is nutrition emphasized? This is not, unfortunately, standard of practice, and it’s still considered something that’s supplementary or extrand with a ketogenic diet, I would say that we are in the midst right now of randomized clinical trials. We’ve just completed a pilot. We have case series. We have case reports. We have observational studies. We have data showing that this is helpful.
We already have our CTs looking at ketogenic metabolic therapies in epilepsy, and that’s been beneficial. We know how it works. Also to some extent, of course, there’s more to be done, but we do know that it’s beneficial for the brain, cognitively also, and we have imaging data to support that.
Why would we not, if something is beneficial also in the metabolic health area, whether it’s obesity or whether it’s insulin resistance? We have that data also, and diabetes, so we know it’s helpful for that. We know that in serious mental illness, there’s high rates of metabolic syndrome or obesity or metabolic issues that we can measure with a simple blood test.
And if we already have that and we know that this is helpful for that, even though we don’t have enough evidence for ketogenic metabolic therapy, specifically for schizophrenia or bipolar illness, but we’re on the way there, then I think the argument is a little bit more in favor of, this is beneficial.
We have a lot of data points here, whether it’s peripheral or coming towards a central closing argument, hopefully, in a couple years, when all the data is out there. But it’s beneficial enough with very low side effect profile compared to drugs that we use, that I don’t think it’s harmful for someone to try it.
What I think is harmful is if someone completely stops their medication and just thinks that, let me start a ketogenic diet and then get off all my medication. No one is following me. There’s no physician following my medication anymore because I made a decision to just get off medication. That’s the part where I think is harmful, and where we need to be more careful in our message.
And there needs to be professional and medical monitoring for this because this is a intervention. It is a therapy. It is not just a diet because it’s so much more than that. It’s like a replacement for a drug in many ways.
Bret:
And now shifting back to Dr. Calkin, who published this groundbreaking study we already mentioned, the TRIO-BD Study, demonstrating that Metformin can improve depression symptoms in patients with refractory bipolar disorder.
So, what does Dr. Calkin hope the impact of this study will be, and how could it change clinical practice?
Cynthia:
I think that the evidence is compelling enough based on our effect sizes, and based on the magnitude of improvement in these patients, who were otherwise treatment-resistant. Because again, this is a population that nothing has worked for decades, and this got patients better in six weeks.
Why wouldn’t you try it? I think that with the study, we do have the evidence. With any study, it needs to be replicated. But I don’t think it’s too soon to be adopting it. I think it needs to be adopted now. What else are you going to use on this patient? Because other psychotropics are not going to get these patients better.
So, why would we keep doing the same thing over and over again when it doesn’t work? We have evidence that this works in treatment-resistant patients, and it works quickly. So for me, it was like a massive because I view myself a clinician first. I stumbled into research, and my collaborator on the TRIO-BD Study in the US, Roy Chengappa, he calls me a closet researcher.
But I think that, I think we need to be looking to what’s going to work. And there’s evidence and rationale behind going after the metabolic dysregulation, and it’s really no different. We test for TSH, we look for hypothyroidism, problems with thyroid in patients who are depressed.
This is really no different. And if they’re hypothyroid, we need to replace them with thyroxine or thyroid hormone. And then, we look at their mood, again, once we’ve treated that underlying medical condition. And so, this is no different. I think we really need to start maybe viewing it that way that might be more acceptable to people.
I think people just struggle with how on earth does insulin resistance or metabolic dysregulation have anything to do with psychiatry and brain disorders? I think that’s where people struggle, and that’s where the understanding that insulin resistance affects blood vessels everywhere in the body and brain.
It causes endothelial damage. And, I think, this is where the link is. So, any brain disorder, Alzheimer’s, Parkinson’s insulin resistance affects these disorders as well. So, I think any brain disorder, we’re going to see that effect.
Bret:
And now let’s conclude with Dr. Sethi discussing if she is optimistic that physicians will soon embrace nutritional ketosis as first line or early intervention therapy for mental illness.
Shebani:
I’m optimistic that this will be adopted and accepted by a large amount of people. Of course, with any kind of new therapy, not everything’s going to be adopted by everybody. Some people may not want to do a ketogenic diet, and I can understand that. But I do think it’s important to be open-minded about what can be helpful for people.
And if it is helpful for a large amount of people or maybe there’s a specific metabolic profile, that it’s helpful for within SMI, I think that’s worth exploring and worth supporting, even if you, yourself, don’t want to do a ketogenic diet. If you see improvements in other people with this intervention as a physician, for example, being open-minded to it, I think is important, and supporting people who want to engage in it is also important.
There’s also a lot of interest in it, especially when you’re struggling with a serious condition. And maybe you have side effects from the medications that you’re on, which limits your availability of what you can try and what you can do and how you can control your symptoms?
If there’s something else out there that has less side effect profile than what you currently have and could even potentially change the dose of what you’re taking to alleviate some of those side effects. As we know, there are side effects for these medications.
Every medication has a side effect. So, it’s always a risk-benefit ratio. And how much of that dose you want to have and combine it with another intervention that has less side effects that can be helpful. It, seems like a no brainer for a lot of people.
Bret:
So, as you hear, the state of the evidence is a complex topic and depends on your perspective.
Are you a treating clinic? Or are you someone looking for care? But the common ground is understanding that there’s a clear association between metabolic and mental health. From there, we can acknowledge the growing evidence suggesting a causative role, although maybe not quite proving it, and other evidence reporting the safety and efficacy of nutritional ketosis.
In a psychiatric population. I’m incredibly grateful to Dr. Sethi and Dr. Calkin for joining us today and sharing their wisdom and experience as researchers and clinicians. And as Dr. Sethi mentioned, there are more trials in the works, as we speak, that will further add to the growing body of literature. So what do you think?
Leave us a comment about how you see the level of evidence, and if it is enough for you to consider nutritional ketosis as a psychiatric treatment. And remember, if you are interested in that topic about medication adjustment and medication management with nutritional ketosis, please watch our dedicated video featuring Dr. Georgie Ede and Matthew Baszucki.
So thank you again for watching, and we’ll see you here next time at Metabolic Mind. I’m Dr. Bret Scher. Have a wonderful and healthy day.
Thanks for listening to the Metabolic Mind Podcast. If you found this episode helpful, please leave a rating and comment as we’d love to hear from you.
And please click the subscribe button so you won’t miss any of our future episodes. And you can see full video episodes on our YouTube page at Metabolic Mind. Lastly, if you know someone who may benefit from this information, please share it as our goal is to spread this information to help as many people as possible.
Thanks again for listening, and we’ll see you here next time at The Metabolic Mind Podcast.
Listen, Watch & Subscribe on:


Disrupted metabolism, so-called metabolic dysfunction, is a dangerous condition that has been associated with numerous medical conditions, including mental illness, dementia, diabetes, heart disease, cancer, and more. What…
Read more
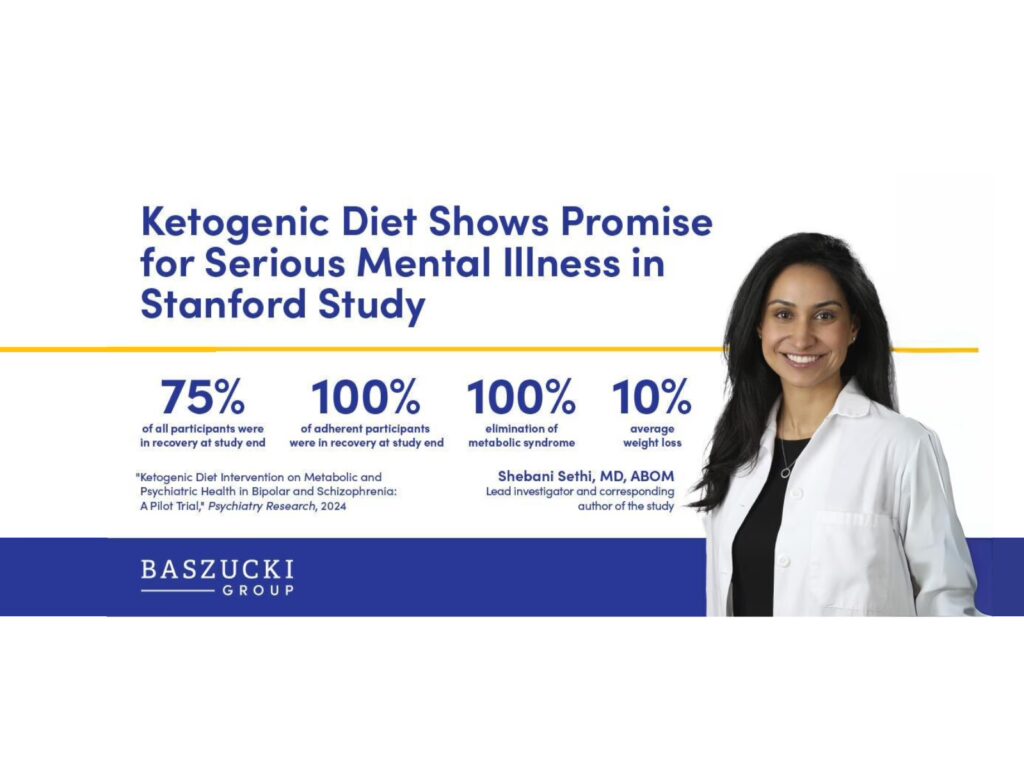
Peer-reviewed clinical pilot trial reports dramatic improvements in psychiatric and metabolic outcomes in bipolar disorder and schizophrenia
Learn more

A Letter From Our Founder
Learn more
Dr. Gordon Guyatt, who coined the term evidence-based medicine, explains its core principles: weighing the trustworthiness of evidence, relying on systematic reviews, and integrating patient values into care. He highlights how small associations in nutrition studies (like red meat and heart disease) are easily explained by bias, unlike the large, undeniable risks seen with smoking. Guyatt stresses the GRADE system as a structured way to judge evidence quality and guide decision-making. For clinicians, this means focusing on when evidence is strong versus when patient preferences must drive care, while the public should learn to distinguish trustworthy from less reliable claims.
Learn more
Disrupted metabolism, so-called metabolic dysfunction, is a dangerous condition that has been associated with numerous medical conditions, including mental illness, dementia, diabetes, heart disease, cancer, and more. What…
Read more
Peer-reviewed clinical pilot trial reports dramatic improvements in psychiatric and metabolic outcomes in bipolar disorder and schizophrenia
Learn more
A Letter From Our Founder
Learn more
Dr. Gordon Guyatt, who coined the term evidence-based medicine, explains its core principles: weighing the trustworthiness of evidence, relying on systematic reviews, and integrating patient values into care. He highlights how small associations in nutrition studies (like red meat and heart disease) are easily explained by bias, unlike the large, undeniable risks seen with smoking. Guyatt stresses the GRADE system as a structured way to judge evidence quality and guide decision-making. For clinicians, this means focusing on when evidence is strong versus when patient preferences must drive care, while the public should learn to distinguish trustworthy from less reliable claims.
Learn more