Get the latest on metabolic psychiatry. Subscribe.

Listen, Watch & Subscribe on:



Does Keto Cause Heart Disease?
Listen
About the host


Bret:
Welcome to the Metabolic Mind Podcast. I’m your host, Dr. Bret Scher. Metabolic Mind is a nonprofit initiative of Baszucki Group where we’re providing information about the intersection of metabolic health and mental health and metabolic therapies, such as nutritional ketosis as therapies for mental illness.
Thank you for joining us. Although our podcast is for informational purposes only and we aren’t giving medical advice, we hope you will learn from our content and it will help facilitate discussions with your healthcare providers to see if you could benefit from exploring the connection between metabolic and mental health.
Does being in nutritional ketosis or following a ketogenic diet increase your risk of developing heart disease? That’s certainly something we hear quite a bit, and many doctors and dietitians believe a keto diet is proven to increase cardiovascular disease. But the reality is there’s no such evidence. So, let me explain.
There are no intervention trials measuring cardiovascular outcomes with nutritional ketosis, meaning no studies have started subjects on a keto diet and found they have more heart disease, heart attack, strokes, et cetera. Not one study has been done to demonstrate this. So, we can’t say with certainty that nutritional ketosis increases cardiovascular events.
Now, to be fair, we also don’t have studies showing nutritional ketosis decreases cardiac events. It works both ways. So, in the absence of outcome data, how do we make sense of all this? It like leaves us in this no man’s land, and how do we know what effect nutritional ketosis may have on our cardiovascular risk?
That would be an important thing to know and to measure. \We have to use what’s called surrogate outcome data, which are results believed to increase or decrease the risk of heart disease. Since we don’t have data evaluating heart attacks or who lives or who dies, we have to fall back on this surrogate data, such as the most commonly used LDL cholesterol.
And while LDL is traditionally the most often used cardiac risk factor, LDL is not the whole story. We should also consider markers of metabolic health, such as glucose, hemoglobin A1C, and insulin, and markers of inflammation, such as CRP, and more specific lipid measures such as ApoB, VLDL, and others.
And don’t worry, I know these are a lot of terms. I just threw a lot of an acronyms and terms at you, but we’ll have a separate video discussing the labs in more detail. So, keep an eye out for that one. But in this video, we’re going to explore the options for evaluating cardiovascular risk with nutritional ketosis, and also talk about some of the evidence people use to falsely believe that there’s an increased cardiac risk with ketosis.
And we’ll talk specifically about the lean mass-hyper responds near the end. So, stick around from that, and really talk about different ways to see this issue. But before we get into the details, please remember our channels for informational purposes only. We’re not providing individual or group medical or healthcare advice or establishing a provider patient relationship.
Many of the interventions we discussed can have dramatic or potentially dangerous effects of done without proper supervision. Consult your healthcare provider before changing your lifestyle or medications. Okay, now let’s start with the existing evidence. Why do some people believe doctors included that low-carb keto diets increase the risk of heart disease?
Many publications or clinicians might cite large observational studies showing that eating more fat or lower carbohydrates increases the risk of heart disease or death. Now, that sounds scary, right? The problem is that most of these studies define low carbohydrate as 40% of your calories.
Or recently, one study made headlines defining low carb as 25% of calories, but we have to understand that is not nutritional ketosis. 40% of calories from carbohydrates on a 2000 calorie diet is 200 grams of carbohydrates per day, and 25% of calories represents hundred 25 grams of carbohydrates per day. That’s more than someone in nutritional ketosis will eat an entire week, let alone a day.
So, the way we can interpret this is that individuals in those studies ate lower carb diets compared to the standard American, the 55% plus carbohydrate diet, but they weren’t in ketosis. So, does that matter? Should we care that they weren’t in ketosis? They ate lower carb. Isn’t that the same thing?
No, absolutely not. It is not the same thing, and we should care whether or not they were in ketosis. Being in ketosis is a physiologic state that changes your metabolism. It’s almost like an on-off switch. You’re either in nutritional ketosis where you’re burning fat for fuel primarily, and you produce ketones, which can also be used as fuel.
Fuel, especially by your brain, or you’re not, right? You’re not in that state. You are or you aren’t. So, being close or closer doesn’t really count, especially in these studies of the general population. So, yes, it does matter whether someone’s in ketosis. Plus, another issue here is that diet quality is essential.
If someone’s eating less than 20 or 30 grams of carbohydrate per day and is in ketosis, it’s tough to fit in processed or sugary foods or the high-calorie, high carb, high fat foods. Compare that to someone who’s eating 100 or 150 grams or 200 grams of carbohydrates per day, lower than the standard American diet, but much higher than nutritional ketosis.
In that setting, those ultra-processed or high-calorie foods containing carbs and fat become much easier to fit in. So, the greater the carb reduction, the lower the risk of adding those potentially concerning foods. And that doesn’t even get into the low-quality data that comes from these observational studies with food frequency questionnaires, which some studies will measure once at the beginning of the study and then never again over 10 years.
Now, does that sound like an accurate way to collect data? Of course not. No, it’s not. There’s also the concept of healthy user bias. The common health message in the 1990s and early 2000s was that low-fat is healthy. So, who was eating low-fat? Generally, those who wanted to be healthier, and those who ate more fat probably weren’t so interested in health advice.
Now, that’s not always the case. But in these studies, it tends to be true for the general population. Those who ate more red meat or more saturated fat also tended to smoke more, drink more alcohol, exercise less, and have other unhealthy life habits. And there are more issues that we won’t get into in this video, but we’ll explore more in dedicated future videos about the difference between observational nutritional studies and randomized controlled trials.
But as you can see, relying on this level of evidence to tell us anything about the health benefits or risks of nutritional ketosis is, I guess, pretty useless at best and potentially incredibly misleading. As I mentioned now, when we don’t have solid outcome data, which we don’t, we fall back on surrogate outcomes, and specifically, it tends to focus on LDL.
So, it’s important to remember though the LDL is only one of many cardiovascular risk factors. Many clinicians believe LDL is not something we should ignore, but it’s also not something we should interpret in isolation. Instead, we should regard it as one cardiovascular risk factor, as I said, and put it into the context of the overall cardiovascular risk assessment and analyze specifically for each individual.
So, here’s one example, which I really like. Virta Health published a paper on their one year continuous care intervention with the ketogenic diet. This was in patients with type II diabetes, looking to treat their diabetes specifically with nutritional ketosis. Now, on average, participants saw their LDL go up by 10%.
However, the 10 year calculated cardiovascular risk went down by 12%. Now, some may see that statistic and wonder how could that be? The LDL went up, but the cardiovascular risk went down. That’s like not what we’re told. It turns out there was no change in ApoB, which is a better marker than LDL. Really, there was a decrease in blood pressure and triglycerides and VLDL and improvement in many other metabolic health markers.
So, according to that calculation, there was an overall reduction in cardiovascular risk. And that’s a clear example of why it’s best to interpret LDL within the context of overall cardiovascular risk. But here’s another issue with assuming that keto increases LDL, and therefore, must increase cardiovascular risk.
It simply isn’t true, right? Multiple meta-analyses show that on average, there’s no net increase in LDL in studies using nutritional ketosis for weight loss or treating type II diabetes. No net increase. Yet somehow, some people, including doctors, believe LDL is bound to go up in everyone starting a keto diet.
The reason that eating that much fat must increase LDL. But as the literature demonstrates, that simply isn’t true. Now that being said, we have to acknowledge there is a population termed hyper-responders where LDL does go up substantially. But again, these tend to be the exception, not the rule. In addition, those with the greatest increase while following a ketogenic diet tend to be leaner and more metabolically healthy.
Engineer and citizen scientist, Dave Feldman, along with Dr. Matt Budoff, Dr. Nick Norwitz and others have published on this topic and are currently studying hyper-responders with a study involving CT angiograms and extensive blood and genetic testing. So, there’s definitely more exciting information to come one way or the other.
Now, Dave Feldman and Dr. Budoff reported their preliminary data at a conference in Denver in February, 2023. On the surface, the preliminary data is really encouraging, but we have to acknowledge it’s only preliminary data. It’s a small sample size and is yet to be published. So, it is too soon at the timing of this recording to say much conclusively about this patient population.
But please understand the lean mass hyper-responders, which we hear so much about are the exception, not the rule. And it’s more common that if someone’s LDL is going to go up, which by no means is a guarantee because most people, it doesn’t remember. But if it does, it’s more likely to go up like by 10 or 15% rather than the 50 or a 100% or more increased seen in the lean mass hyper-responder population.
Okay, so now we’ve reviewed the lack of outcome data, the faulty and misleading observational data, and the caveat of the lean mass hyper-responders. But now, we’re at this place wondering, where does that leave us? How do you, as an individual or a clinician, know what to do regarding nutritional ketosis, LDL and cardiac risk?
We can see this as two ways there. There are two potential ways to approach this question in my mind. The first is that since no outcome data exists on those in nutritional ketosis, then they should be treated just like everybody else, even though they’re metabolically different, and their dietary makeup is drastically different from the general population.
Many physicians prefer caution until more definitive data exists. So for them, guideline medicine still applies. But the other approach is that since this population is clearly physiologically unique, they should be treated differently. This population should have its own guidelines that reflect their metabolic health and unique physiology of being in ketosis.
Now, this isn’t evidence-based, but neither approach really is for that, for this specific population. At this point, we can’t say which is right or wrong. These are preferences reflecting the opinions of both the provider and the individual. But either way, I think it’s still crucial not to use LDL as a solitary measure or to ignore it entirely either approach. But instead, to factor it into the overall health and benefits the in individual has achieved through nutritional ketosis.
Now, speaking of benefits, this is a crucial point to make. We have to know the benefits the individual has seen through nutritional ketosis. In a prior video, I was somewhat critical of Dr. Christopher Gardner, who was quoted in an article saying the risks of a keto diet outweigh the benefits. Of course, first, he wasn’t even talking about a keto diet.
This was the keto-like diet study with 25% of calories from carbs. So, it’s entirely off-base to begin with, but my biggest problem is this. How does he know what the benefits even are? How can he say the risks outweigh the benefits when he has no idea what benefits in individual experiences?
Understanding the benefits to the individual is crucial to interpreting the risk-benefit ratio. What if someone had decades of anorexia with absolutely no improvement, except for when they started nutritional ketosis? That’s pretty crucial to know. Or if someone has struggled with finding adequate treatment for bipolar disorder, and nutritional ketosis help put their symptoms into remission?
That has to weigh heavily on your decision as you evaluate a risk-benefit ratio. What if someone put their type II diabetes into remission? How would that change your perception if their LDL went up by 10 or 15% or even 50%? Again, I’m not sure there’s an automatic answer to whether that’s good or bad, but it needs to be individualized.
And that word, individualized, exemplifies where medicine should go. Of course, we should be individualized for each patient, but unfortunately, busy doctors tend to want to use guidelines, and our medical practice tends to encourage treating people similarly, I guess you can say. But that’s a trap I hope we can avoid by continuing to discuss the unique physiologic state of nutritional ketosis.
So, how do we answer the question? Does nutritional ketosis increase cardiovascular risk? The answer is we don’t know, at least not from concrete outcome studies. And even with surrogate studies, there’s still no convincing evidence. We have to acknowledge there’s a small population where LDL can go up dramatically, and we shouldn’t take that lightly.
Rather, we should factor it into the patient’s overall health and overall progress, or their reaction to nutritional ketosis. And we need to deeply understand the benefits for each individual to be able to factor in a risk-benefit ratio. But I think it’s clear, the evidence does not support the automatic assumption that nutritional ketosis increases cardiovascular risk or even automatically increases LDL.
And changing this mindset is crucial so that clinicians might be more willing to try nutritional ketosis as a therapeutic medical intervention, especially for those who have tried multiple different interventions for their type II diabetes or their Alzheimer’s disease or their psychiatric condition or other health issues.
If a doctor falsely believes keto will cause a heart attack, of course ,they’re going to be hesitant to recommend it. But if they knew the potential benefits and knew that there was no evidence showing increased heart disease, then they’d be much more willing to consider nutritional ketosis as a therapeutic intervention in the right setting.
So, what do you think? How do you see the issue of cardiac risk with nutritional ketosis? Leave us a comment as we would love to hear your take on this issue. And if you found this video helpful, please click the thumbs up and subscribe buttons so you won’t miss any of our future content. And please share this video with anyone you think may benefit, including your physician.
And if you want to understand the potentially profound effects of nutritional ketosis on mental health, please watch this incredible story of one family’s reversal of dementia and regaining their lives back after beginning nutritional ketosis. And keep an eye out for our future video of what you can do about elevated LDL while in nutritional ketosis, which sort of ties into this whole concept of cardiovascular risk and whether LDL is important or not.
But there are tricks you can do to manage it and maintain nutritional ketosis. Because for some, the importance of being in nutritional ketosis outweigh any potential changes in LDL. So, thank you for watching. Thank you for listening. I’m Dr. Bret Scher, and I look forward to seeing you again here next time at Metabolic Mind.
Thanks for listening to the Metabolic Mind Podcast. If you found this episode helpful, please leave a rating and comment as we’d love to hear from you. And please click the subscribe button so you won’t miss any of our future episodes. And you can see full video episodes on our YouTube page at Metabolic Mind.
Lastly, if you know someone who may benefit from this information, please share it as our goal. Is to spread this information to help as many people as possible. Thanks again for listening, and we’ll see you here next time at the Metabolic Mind Podcast.
Listen, Watch & Subscribe on:

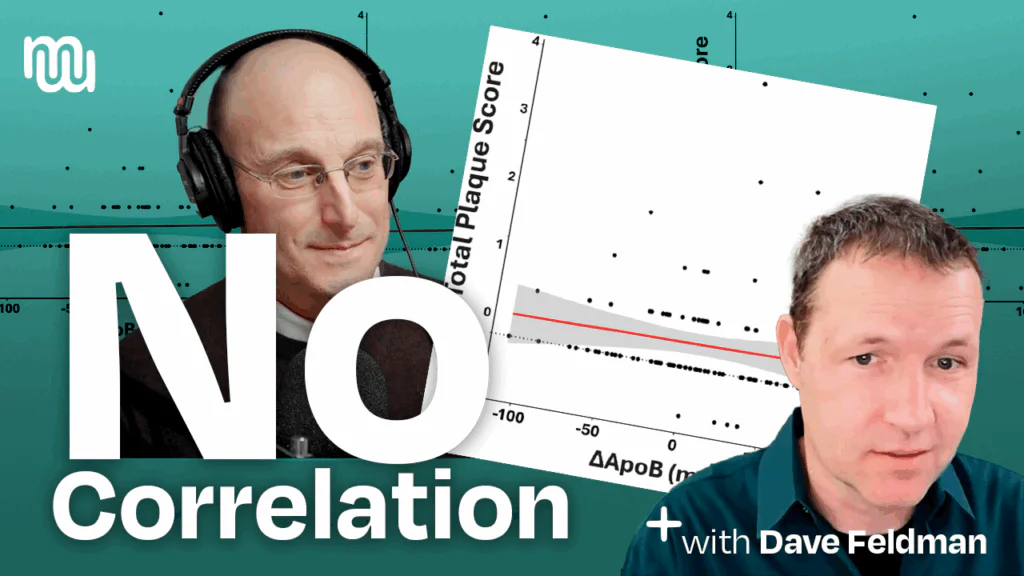
Engineer-researcher Dave Feldman walks through the lean-mass hyper-responder (LMHR) keto-CTA trial: 100 metabolically healthy keto eaters with very high LDL/ApoB had coronary CT angiograms at baseline and ~1 year. Key finding: changes in plaque (including non-calcified plaque) did not correlate with LDL or ApoB; the best predictor of progression was pre-existing plaque. Keto itself wasn’t shown to drive plaque, and saturated-fat intake and cumulative on-diet LDL exposure didn’t track with ApoB or plaque change either. Plaque did rise modestly for some—about what’s seen in treated cohorts—while a few even regressed; interpretation should be individualized with imaging (CAC/CTA) guiding care and standard therapies used when plaque is present. Limitations (e.g., no longitudinal control group) mean more studies are needed; Dave’s team is launching follow-ups and invites open, civil debate—“don’t confuse arsonists with firefighters.” Resources: CitizenScienceFoundation.org and cholesterolcodemovie.com.
Read more
This episode features cardiologist Dr. Matt Budoff on a one-year CT-angiography study of lean, keto-adhering “hyper-responders” with very high LDL/ApoB. Headline finding: no clear link between higher LDL/ApoB and coronary plaque progression; instead, baseline plaque burden predicted who progressed. Some participants even showed plaque regression despite LDL >200 mg/dL, underscoring wide individual variability. Takeaway: ketogenic diets weren’t shown to accelerate heart disease; use CAC/CTA to assess plaque and treat existing atherosclerosis per standard care, independent of diet.
Learn more
Cardiologist Dr. Matt Budoff returns to explain how coronary CT metrics—especially percent atheroma volume (PAV) and non-calcified plaque—should be interpreted in the new lean mass hyper-responder study. He clarifies that plaque did progress in some participants, but the rise was similar to treated cohorts in other trials and was not linked to keto-induced LDL or ApoB levels. The episode unpacks why relative percent changes can mislead when baseline plaque is tiny, and why calcium score/CTA help distinguish low- from higher-risk individuals. Practical takeaway: keto wasn’t shown to drive plaque; use imaging to check for atherosclerosis and treat documented plaque per standard care, independent of diet.
Learn more

In this video, board-certified cardiologist (and Metabolic Mind’s Medical Director) Dr. Bret Scher dives into the latest science of triglyceride-rich particles and their impact on metabolic health. Learn…
Learn more
Engineer-researcher Dave Feldman walks through the lean-mass hyper-responder (LMHR) keto-CTA trial: 100 metabolically healthy keto eaters with very high LDL/ApoB had coronary CT angiograms at baseline and ~1 year. Key finding: changes in plaque (including non-calcified plaque) did not correlate with LDL or ApoB; the best predictor of progression was pre-existing plaque. Keto itself wasn’t shown to drive plaque, and saturated-fat intake and cumulative on-diet LDL exposure didn’t track with ApoB or plaque change either. Plaque did rise modestly for some—about what’s seen in treated cohorts—while a few even regressed; interpretation should be individualized with imaging (CAC/CTA) guiding care and standard therapies used when plaque is present. Limitations (e.g., no longitudinal control group) mean more studies are needed; Dave’s team is launching follow-ups and invites open, civil debate—“don’t confuse arsonists with firefighters.” Resources: CitizenScienceFoundation.org and cholesterolcodemovie.com.
Read more
This episode features cardiologist Dr. Matt Budoff on a one-year CT-angiography study of lean, keto-adhering “hyper-responders” with very high LDL/ApoB. Headline finding: no clear link between higher LDL/ApoB and coronary plaque progression; instead, baseline plaque burden predicted who progressed. Some participants even showed plaque regression despite LDL >200 mg/dL, underscoring wide individual variability. Takeaway: ketogenic diets weren’t shown to accelerate heart disease; use CAC/CTA to assess plaque and treat existing atherosclerosis per standard care, independent of diet.
Learn more
Cardiologist Dr. Matt Budoff returns to explain how coronary CT metrics—especially percent atheroma volume (PAV) and non-calcified plaque—should be interpreted in the new lean mass hyper-responder study. He clarifies that plaque did progress in some participants, but the rise was similar to treated cohorts in other trials and was not linked to keto-induced LDL or ApoB levels. The episode unpacks why relative percent changes can mislead when baseline plaque is tiny, and why calcium score/CTA help distinguish low- from higher-risk individuals. Practical takeaway: keto wasn’t shown to drive plaque; use imaging to check for atherosclerosis and treat documented plaque per standard care, independent of diet.
Learn more
In this video, board-certified cardiologist (and Metabolic Mind’s Medical Director) Dr. Bret Scher dives into the latest science of triglyceride-rich particles and their impact on metabolic health. Learn…
Learn more