Share your story. Help someone else start theirs. Share Now

Listen, Watch & Subscribe on:



College Mental Health Crisis: How Students Can Combat Depression & Anxiety
Listen
About the host

About the guest

About the guest

About the host
About the guest
About the guest

Drew:
If we can encourage those kinds of clubs to get started at the different universities, that will really help out, not only by sticking to the diet, but also by building community, which is extremely important.
Bret:
That’s a great suggestion.
Georgia:
I love that you make keto cool.
Drew:
Absolutely. It is cool.
Bret:
It is cool. If you’re going to college, in college, or if you have a loved one in college, you’ll want to hear this interview.
College mental health is a great concern, and it’s a perfect storm of independence, lifestyle changes, and stress that can lead to a number of mental health concerns. But there is hope, and there’s a lot that can be done about it, including nutritional interventions, and I’m joined today to talk about that.
I’m joined by Dr. Georgia Ede, who is a board-certified Harvard-trained psychiatrist who spent years specializing in college mental health, and also Drew Decker, who is a graduate research associate at the Ohio State University with Dr. Jeff Volek in his lab, and also a US Army veteran, which plays into his experience and his interest in nutrition and ketosis for mental health.
And so we’re going to explore the many aspects of collegiate mental health and some of the results from the groundbreaking kind study that Drew Decker was involved in, and how that can maybe inform what we can be recommending and how we can help support college-age individuals with making better lifestyle choices.
So I hope you enjoy this interview with Dr. Georgia Ede and with Drew Decker. Drew, welcome. Thanks for joining me and Georgia here on Metabolic Mind. It’s great to have you.
Drew:
Thanks for having me, Bret. It’s great to be here.
Bret:
I am really interested, very interested, I wanna get into the details with both you and Georgia about nutritional interventions in college-aged populations and specifically ketogenic interventions.
But before we do, give us, a little bit of your background, how did you get here? What got you interested in college mental health, nutrition, and ketosis? How did all that come about?
Drew:
Yeah, Bret, that’s a great question. As far as my interest in ketosis is concerned, I was a former military member, an airborne paratrooper, and I ended up suffering a massive TBI during training.
And so I had recurring migraines. I ended up hearing that the ketogenic diet could be a treatment for some of those symptoms. And I heard Dr. Volek actually give a speech during my undergrad. Talking about what his lab does and the different potential implications of a ketogenic diet or different chronic diseases.
And I got extremely interested in it. So I tried the ketogenic diet out, and I ended up reducing my occurrence of migraines from once to twice every week to once every couple of months. And even then I could still work through it. So I was really committed to that as far as my interest in it with mental health is concerned.
When I hit my head, I ended up having a lot of anxiety issues. I almost had a bit of a, not quite a personality shift, but I definitely had issues that I never had before. And I was going through bouts of depression. And so one of the things that I noticed is once I got on a ketogenic diet, had a lot of things became a little bit easier to handle than they were before.
So this already had me very interested in it. And so when Dr. Bowl came up and said, Hey, I have this opportunity to. Look at the effective ketogenic diet on mental health. I took it and ran with it. Did not wanna look back.
Bret:
Wow. Yeah. That’s an incredible story. And it’s always inspiring to me when people take their personal experiences, their personal struggles and successes, and then turn it into to research, to science, and eventually to clinical practice.
I just think that’s so incredible and gives you more skin in the game and more passion, so I really appreciate that. And Georgia, I want to hear about your background in. In student mental health and college mental health, because I know you spent a lot of years in that realm too. So tell us about that.
Georgia:
Yeah. I actually specialized in college mental health coming out of residency I’d done a fellowship in college mental health at Harvard, and then eventually worked at Harvard University Health Service for seven years as a college psychiatrist, and then at Smith College in Western Massachusetts for five years.
And that was really my first love was college mental health. And as I think we’ll get to talking with Drew about it can be very challenging. The food environment on college campuses can be very challenging in terms of trying to help students, encourage students to eat a brain healthier diet.
And so that was one of the reasons why ultimately had to leave my beloved specialty of college mental health so that it could really fully engage. With nutritional and metabolic interventions in my work. So I’m really looking forward to this discussion because there are some real challenges on college campuses when it comes to the culture of food and all the stress that students are under.
But yes it’s, this is a topic really near and dear to my heart.
Bret:
Yeah. And I think that sets it up really well about the challenges that need to be overcome in this particular population. And Drew, you were very involved in the kind trial which was a intervention, a ketogenic diet intervention for college aged students with depression.
So clearly a focus on depression. But Georgia, what are some of the other main diagnoses or, mental health struggles that you saw? In your career in college mental health?
Georgia:
Well, college mental health is really a time of extraordinary vulnerability to all kinds of mental health problems. Really everything you can imagine is you would see.
On a college campus. So everything from A DHD, mild depression, anxiety, panic attacks, PTSD to severe major depression, suicidal ideation, suicidal behaviors, self-injury psychosis bipolar disorder substance abuse. Really everything that you can imagine is present on college campuses because that is a time of life of special vulnerability.
In addition to the age of life being a vulnerable time, it’s also many students have moved away from their families, from their homes, sometimes across halfway across the world to to enter this pressure, co academic pressure cooker and people can really isolated. It’s a extraordinarily stressful time.
It’s, it really was. I, I. I often say this, and it’s, I, sometimes I hesitate to say it, but it simply is the truth that working as a psychiatrist in a, an ecology university setting, it often felt like working in an emergency room. Because there were small Benny crises that would come in every day.
Students needing leaves of absence students needing special support, students needing hospitalization medication management. So this is a very serious problem and why I am so excited to hear more about the kind study when it gets released to find out what’s possible when we have really good support for what I consider to be.
A nutritional intervention with tremendous potential.
Bret:
Yeah. Yeah. So Drew we’ve mentioned the kind study a couple times now, and I know at the time of this recording, it’s not officially published, but tell us what you can about the impact of a ketogenic diet on these selected individuals, which granted, as with any research study, there were inclusion and exclusion criteria.
So what was the impact on these individuals with depression?
Drew:
I don’t want to overstate or understate this. The first the primary focus of the study was to show feasibility of the diet, which we did. The individuals that were that through the study we’re able to maintain a state of ketosis stay in nutritional ketosis.
And that was despite a lot of the challenges they had, again, food halls, college food, so on and so forth. So we’re able to show that, but I think. More importantly was we were able to show decreases in their symptoms of depression pretty early on, within as early as two weeks to the point where most of these individuals, a lot of ’em, would not even be considered clinically depressed anymore at the end of this throughout the two weeks so that these benefits were actually seen throughout the remainder of the study.
It was a 12 week intervention. So I think that’s probably the key takeaway here is that, I don’t wanna overstate this, but we are changing lives with with diet, again, this stu this study was done alongside of counseling and medications on and so forth, but still the effects that we were seeing was absolutely amazing.
And the feedback that we were getting from students was incredible. We had students coming up saying they were able to handle situations they never could in the past. Just the amount of positive feedback we got. We have a lot of the individuals that are continuing on the diet even though they’re no longer in the study.
Even one that was saying she got her parents to get onto the ketogenic diet at this point ’cause she was such a believer in it. Very positive outcomes.
Bret:
Yeah. Georgia, how do you react when you hear that about the dramatic impact that, that a ketogenic diet had?
Georgia:
I got music to my ears, of course.
And Brett and I were both at a conference last year where we heard some of the preliminary data, which we can’t share with everybody, but it was really exciting to see those preliminary results and I can’t wait to see what you’ve put together for, with the published report.
It really is. So encouraging to me to hear this, especially where you have students telling you that they wanna continue with the diet beyond the study, because that’s always the criticism that we hear when we mention positive results from a mental health study about the ketogenic diet. Okay.
That. That’s great. I’m, I’m glad that, that helped those people during that period of time, but no one’s gonna be able to stay on it. Nobody’s gonna wanna stay on it. Nobody’s gonna enjoy this diet. So you know why it really doesn’t matter in the long run if you can’t adhere to it.
Bret:
Are you surprised that there was such good adherence, actually, both of you? Was it a surprise that there was such good adherence. In this population with the challenges that you alluded to already Georgia about, living on their own. The food options aren’t so great. And it can be very limiting in time and stress and whatever.
People aren’t often paying attention to how well they eat.
Drew:
Personally, maybe I’m just a forever optimist here, but I was not very surprised that individuals are able to stay to the diet again, with my own personal experience with it, once you start to feel these effects like. How could you stop?
It’s one of those things where it makes it worth it. And as far as like enjoyability and palatability of the diet you’re eating a lot of high-fat foods. It’s a very enjoyable diet. You just have to figure out what fits with you and what you personally like, which is something that we would help individuals with is just how can we personalize this diet to you?
So we had individuals coming in saying, Hey, I actually enjoy this diet more than I did, when I was eating. Fast food every day or whatever, so I was I wasn’t very surprised. I figured that this was gonna take and stay.
Georgia:
Drew, I’m wondering what kinds of challenges so it it sounds like some students really took to the diet and are going to be continuing it longer term and it even has a contagious effect on some of the other people in their lives, which we see all the time.
But what were some of the challenges socially on campus, families, friends and a dining hall culture? I’m very curious to know what were some of the hardest things you faced in this small study?
Drew:
Yeah, so I think one of the biggest issues that we had was the social aspect of it specifically with family, right?
So we had several family members that were. Right? But they hear they’re gonna be eating a lot of saturated fat. So a lot of times we’d have parents chiming in saying, no, that’s not healthy. We can’t do that. And so that we try to send, information to the students, that way they can get it to their parents, and try to calm them down.
But there was a lot of misinformation that was just being put on them and scaring them. And then also individuals are apprehensive to go on vacation. You’ve got Thanksgiving coming up or you have Christmas coming up. So sometimes around those holidays there’s a lot of apprehension on how to handle that.
And, we would give the best advice that we could and. A lot of times, a lot of times they would leave saying, Hey, I might not be the most adherent to this diet while I’m on vacation. And my advice was always, okay, that’s fine. We want good is not, the enemy is of perfect, right? Good is still good.
So we want to, if you do come off, that’s fine, just come back on. And we’ll figure it out. But a lot of times they would leave and they’d, you’d look at their ketones and they’d never even go down. So you’d see individuals that were staying on throughout the holiday as well.
A lot of the things that I thought were gonna be really big issues weren’t as bad. You mentioned dining hall issues. One of the, one of the advices that we have is for OSU, for Ohio State University, there is a dining website that you can go to that has nutrition facts of the foods that they’re supplying.
So there you can direct individuals like, Hey, there’s a lot of variety at these. These dining halls and you can make a choice that fits within the ketogenic diet, even though you’re eating off of college food and off of, your Buckeye Pass or whatever they call it, at whatever university.
We were able to really mitigate a lot of the issues we thought we were going to have.
Georgia:
That’s a great way to reframe it because the, as dining hall choices on campus, in some ways people have more choice there than anywhere else. The places that I worked, there were vegan dining halls.
There were dining halls for athletes that had extra carbohydrates. There were, vegetarian dining halls. There were kosher dining halls. What you couldn’t find was a Whole Foods dining hall. You couldn’t find any kind of dining hall that just served healthy Whole Foods quit or not.
And but to emphasize that, yes, you’ve got this buffet of, all kinds of food every day, including dessert, very sweet dessert like foods at breakfast, lunch, and dinner. But that doesn’t mean you have to choose those. So I think that’s a new way to reframe it.
Drew:
I feel like if there’s a variety at a restaurant or dining hall, then.
You are always able to make a ketogenic option. It doesn’t matter where I go out to eat. I’m able to find something that fits within my diet.
Bret:
Yeah. And that goes back to just the education, like really showing people and breaking down that sort of. Barrier that people may have right away, which often is just rooted in misunderstanding.
Which, which leads me to a question about the family, which I thought was so interesting that you brought that up, drew, and here we’re talking about individuals who are over 18, right? They are considered adults, they can make their own decisions and give their own consent and so forth. But Georgia when you were working with individuals with, the numerous different mental health challenges that, that you listed.
How much of it was working with the individual working versus working with the family and trying to get to the. The right course of treatment for the individual because the individual’s, your patient, not the family, but the family obviously has a very vested interest. So how did you balance that?
Georgia:
I did very little work with families. I worked mostly one-on-one with students. The pushback that I would get wasn’t from family members. It was more from wellness directors and dieticians on campus who who believed in, would even meet with me to tell me that, the brain needs 130 grams of carbohydrate per day.
That even encouraging students to eat less sweets fewer refined carbohydrates. We’re not talking about starting college students on a ketogenic diet. That’s not what I was doing with most students. We’re just trying to reinforce healthier eating habits. By choosing against certain foods. I was told that would encourage eating disordered behavior, that everything should be in moderate, in, in moderation.
And that and that it, they were really discouraging me against counseling students about how to eat healthier. So some of that, some of the pushback came from administration. And drew, I’m really curious to know, did you face any of that and also. The other piece of college culture, food culture, which I found very frustrating was there were wellness events that were, students would be lured to wellness events with cupcakes, with ice cream, with cookies, pizza parties where trying to get students to come to these.
Wellness oriented events that were actually, of course very dangerous for their mental health. So was there any administrative concern about what you were recommending for students?
Drew:
I know Georgia, luckily for us we didn’t really have any pushback that I was aware of, at least administratively.
We also had a great psychiatrists and psychology team that were working with us and they were all on board. So they’re, all about going for the ketogenic diet. So I think that, maybe one of the benefits that we had on this was that lack of pushback from administration. So it’s not like our participants were really getting a lot of, influence inside of the university to stop with the diet, at least that we were aware of.
But yeah I see the same problem with all the wellness events are always pushing. Foods that are the exact opposite of what you should be pushing for. For health.
Bret:
Yeah. And I think maybe in the setting of a research study is maybe a little bit different than trying to, give the treatments or give the recommendations on a broader scope.
But hopefully this will help start to push things in that direction to say, okay, maybe this is more acceptable. And one of the other challenges with college age individuals that we have to acknowledge is alcohol. And that can obviously contribute to depression symptoms and be involved with that.
But on a ketogenic diet, you do have to be careful about alcohol, specifically high carb alcohol, like beer. So how about how did you handle that and was there concern from the individuals?
Drew:
Yeah. We’ve all been to college here, right? We have that, there’s that social pressure for drinking and.
A lot of your friends are going out and they’re gonna be consuming alcohol, and you don’t wanna feel like you’re left out. So the way that I handled this was I didn’t say you can’t drink per se. I gave more information as to what kind of alcohols you wanna avoid what kind of alcohols you can get away with, is the way I’ll say that.
And then I also made sure I gave information as to what really occurs when you’re drinking as far as endogenous production of ketones, right? So even though you’re drinking an alcohol, that might not kick you out of ketosis, it’s also going to slow down your own production of ketones, which might have a negative effects long term, right?
I never really need to tell anybody they couldn’t do something. Especially if that was a part of their, I don’t wanna limit their social interactions. Those are still very important. But I just wanted them to know exactly what they were getting into if they decided to partake with alcohol.
And again, it was, I had a huge philosophy throughout the entire event, which was good is not the enemy of perfect. So if you make that mistake, that’s okay. That’s fine. Just get back on the horse and we’ll just keep on going after that.
Georgia:
Drew, I’m really curious, did you have any trouble recruiting for this study?
Was there a lot of interest in it, or were, was it hard to find students who were interested in doing this?
Drew:
Yeah, Georgia, that’s a good question. Recruitment was a little bit slow for us, and I think a lot of that had to do with just how stringent we were on our recruitment. We wanted individuals to already be going through, treatment that we wanted them to have a diagnosis of major depressive disorder and we wanted them to come through a certain within a certain range of OSU campus with where they’re finding, being their primary care provider. I think those were the main stoppers for us when it comes to what our recruitment material was, why things were slow for us to recruit.
As far as interest, I think there was quite a bit of interest for getting onto this. Again, you have students that are struggling, right? They’re having, dealing with mental health issues. If you have depression, you largely feel alone even when people are trying to reach out and trying to help you still feel alone.
You feel like you’re in it by yourself. I think a lot of people that are suffering are looking for answers. They’re looking for a way. So if you’re providing, hey, we’re studying this, we’re giving this possible intervention to potentially help with depression, I think a lot of students are willing to jump onto that and, just try something.
Georgia:
Yeah. And and did you, were the students who volunteered for your study, how was their metabolic health in general?
Drew:
Honestly, their metabolic health, they all seemed pretty insulin sensitive, which is good. It was surprising at first. ‘Cause we had, body compositions all over the board, and we had tons of different individuals. So we were very surprised to see that pretty much everybody was insulin sensitivity sensitive. And I don’t think I was a byproduct of them being. Making the best dietary choices. I think that was just a byproduct of them being young and their dietary choices hasn’t, haven’t caught up to them yet.
So they’ve been able to get away with it up until this point. So it was actually surprising. That was one of the things we didn’t expect to see was everybody came in pretty metabolically healthy from the start.
Bret:
Yeah, with this age of a population, you’re probably less likely to see overt metabolic dysfunction, although that trend is certainly starting to change.
As we see more and more pediatric obesity and pediatric metabolic dysfunction. But how about you, Georgia? Did you encounter a lot of metabolic dysfunction in the individuals you were treating for mental illness?
Georgia:
Yes. So there was a lot of overweight and obesity on the campuses that I worked at.
And more as each year went by, right? So it seemed to be, the problem seemed to be getting worse before our eyes with every passing year. And there were time, I was eventually measuring fasting insulin levels on students and we had fasting insulin levels on some students in the thirties and forties.
And some students already in the pre-diabetes range with their glucose levels and so forth, students by and large, their metabolic health, it varied a lot, but there were certainly many students with very poor metabolic health. But I also had students who on the surface appeared to have really robust.
Physical and mental health, even, star athletes on campus who are nevertheless struggling with very, severe depression. Speaking to the fact that physical fitness while very important isn’t always enough to keep people well. So another thing I’m wondering about, drew, I don’t know if you’re, if you can speak to this or not, but how many students were taking.
Already taking antidepressant medication. When they enrolled in the study,
Drew:
Honestly, the majority of our students the participants were not on medication. We had a subset that were on medication, and I think the interesting takeaway from this was that despite medication status, we still saw similar improvements in symptoms of depression, which I think was absolutely incredible to see.
But. We did have individuals that were taking some medications mostly selective serotonin reuptake, inhi inhibitors. But yeah, it didn’t really seem to change the result, the outcome whether they were on or not.
Bret:
You, already mentioned that this was in addition to the treatment they were getting, right?
It wasn’t a brand new treatment. These were patients already with a diagnosis who were in the system, so to speak, who were undergoing some sort of treatment. Is that right?
Drew:
Correct. Yeah. This was adjunct to standard of care. So again, one of the preliminary or one of the inclusion criteria was that the participant had already been involved.
And counseling program, whether that just be psychotherapy or pharmac cotherapy.
Bret:
And it goes back to the etiology of depression, the mechanism of depression, or I should say etiologies and mechanisms. Like it’s not just one thing, which you and I Georgia have talked about quite a bit, but as you set it up, here’s someone they’re living on their own PO probably for the first time, they’re, they have the increased stresses of the academic. Institution and introduce, potential alcohol and drugs and. Poor sleep habits and, it’s not one thing that’s causing, quote unquote the depression or the psychiatric symptoms. So it’s probably not just one treatment that’s going to take care of all of it.
So how would you balance sort of the role for. For therapy and understanding the new situation versus the role of medications versus the role of nutrition and like trying to pile all that on someone who’s already stressed, who’s already trying to, do their homework and be social and time constrained.
How would you balance that?
Georgia:
No, it’s true. So there are, this is really the. I was talking before about the pushback, the administrative pushback, but of course then does the students themselves pushing back, right? So students themselves saying it’s, I’m already under so much stress, it’s already too hard to manage everything I’m trying to manage, and now you’re asking me to make one other change.
I just can’t, I can’t do it. And a lot of students. You can hear it in when you’re talking with them. And they’ll even sometimes come right out and say, I’m a carbo holic. I need these foods. I turn to these foods when I’m stressed. I don’t know, how else am I gonna manage my stress if I can’t lean on these foods that give me comfort?
And so this was a really, the food addiction piece with a carbohydrate addiction piece was a major barrier to being able to. To be successful with dietary changes on the college campus. It’s also the age group. It’s very important for young people, emerging adult teenagers and emerging adults to feel part of their group and to do things together the same way.
In order to be accepted. It’s really hard for students to make friends when they first get on campus and now you’re gonna add on to now I eat this strange diet and so I, I can’t go have pizza with, with this group of people at one o’clock in the morning. So it was a, it was, again, that was a major reason why I left college mental health was because of those barriers, but I didn’t have the infrastructure that you have drew with this.
With the team approach that I’m that I understand you use and I’m really curious to know how much do you think it would take to offer this kind of a service to students on a college campus? Would it cost more than what the dining halls and the counseling centers are already providing?
Logistically, how would that work? Because I, I know a lot of. Administrators will say I’m fine. It works, but we don’t have the money, we don’t have the resources. We’re already strapped. We don’t have enough counselors, we don’t have enough psychiatrists. We don’t have enough hours to see all these students who are really struggling, and now you’re asking us to add another service on top of what we’re an already stretched service.
Drew:
I think I’d reframe it to say, I’m not asking you to make another service. I would say that just trying to. Be more forthright with the foods that are being offered. So I, like I said, you can go to these websites OSU dining or whatever, and you can find the nutrition info for that’s being offered here and individuals can go to that.
But again, that requires a baseline knowledge that isn’t very advertised. It’s not advertised at the university level. And I think. The education piece as far as where you can find this nutrition information needs to be pushed out a little bit further. So my, my argument wouldn’t necessarily be we need to change what’s at the dining hall.
It’s just more we need to advertise what is at the dining hall a little bit better. And same with with the point of, hey, I, I have my comfort foods that I like. A lot of ketogenic. Our keto friendly foods are out there that are pretty good replacements, pretty good one-to-ones.
You can even find noodle replacements at this point that are pretty good. It’s just a matter of getting the information out there. Having that education piece. You can have your comfort foods, you can have, your sweet treat every once in a while. You just need to make the right choice as far as which one you’re getting right.
And so that’s just more of an education piece. When it comes to that. So we were able to have individuals that were, like I said before, they were absolutely addicted to noodles. That’s all they wanted to eat. We found them a keto friendly noodle and they were able to stay within a nutritional level of ketosis throughout the entire thing or throughout the entire intervention and.
Had their noodles every day, so they stayed happy.
Georgia:
Were they making these noodles in their dorm rooms? How were they cooking the noodles?
Drew:
Yeah, so they only required, a microwave or whatever, so it wasn’t too hard for them. We also had a lot of grad students that were also in, so some of them weren’t necessarily living in the dorms.
A lot of ’em were able to, have their own apartment and so they’re able to cook on their own as well, which led into a whole nother piece on education for what? You should shop for and, financially friendly options that you can get at the grocery store, that fill within a ketogenic diet.
Bret:
Yeah, and that’s a great point. We’ve been talking about it at least in my mind, framing it as if people are living in the dorms and in, going to eat at the food halls. But many colleges you’re lucky to be on, on campus in a dorm your first year, and then the rest of the time you’re in.
You’re in an apartment and sometimes you’re in an apartment all four years depending. So that’s the other aspect that the shopping and the cooking or knowing which fast food places to go to, where you’re going to, where you’re gonna be able to do it. So yeah. Another part of the education and going back to the dining hall is, my guess is they have a vegetarian option or vegan option.
They my, my guess is most places have that option because it’s just more socially acceptable. But now. With the evidence that you’re providing from your study, it seems like schools should also be offering a low carb option, or Georgia, like you said, a Whole Foods option, which shouldn’t be that much more difficult to offer that option as well.
Do you have hope that could happen?
Drew:
Yeah, I think we’re almost there. I think we’re like halfway to it because right now I think it, a student can eat a Whole Foods or a ketogenic diet. Had the dining hall, as long as they know what they’re doing it would be nice if they had it lumped into one section.
But right now, I think if the cheapest way moving forward and probably the most realistic for the short term would just be to increase the education piece. Maybe have. Color system or something at the university where they can, green equals low carb option or something like that, and they can just have that set up next to each food.
But yeah, I think it’s very doable.
Georgia:
That’s a fantastic idea. And that way students have a choice and they’re supported in this, these very subtle, simple, inexpensive ways. To be able to follow the meal plan of their choice. The other piece of that question that I wanna understand more about is, I know in your study one of the keys to helping people transition onto this diet was support and being able to access somebody through an app who could answer questions about the diet and help them troubleshoot.
And so that, that piece of counseling do you think that would be important to supporting students maybe trying to do this in the future? Or do you think there’s a way for this to work without that element?
Drew:
I think it would be beneficial for everybody that’s suffering from mental health, trying to go through or stick the ketogenic diet to have.
Some kind of support. So ideally we’d have the clinicians that are trained up and at least understand some of the basic guiding principles of a well-formulated ketogenic diet. That would be the ideal situation. But even if we could set up, or even if, students could set up.
Their own clubs, right? Ketogenic friendly club or something like that. Somewhere where they have their own community that they could just talk with each other. Hey, I’m about to eat this. Does this fit with what you guys have done? Have you had this? What are your ketone levels usually at after you eat this?
Universities are filled with clubs, with student ran clubs and if we can encourage those kind of clubs to get started at the different universities that really help out with not only sticking to the diet, but also building community, which is extremely important.
Georgia:
That’s great, I love that you make keto cool.
Drew:
Absolutely. Absolutely. It is cool. It is cool.
Bret:
Drew and Georgia, I want to thank you both so much for your contributions to this really interesting discussion. Clearly such an important topic with the challenges that so many college age kids can face from a mental health standpoint but.
Optimistic that there’s so much that can be done about it. So thank you both for your contributions and Drew, I look forward to you exploring the results of the study more when it’s published because it sounds like so dramatic for the impact it can have for individuals. So thank you so much.
Drew:
Yeah, thank you Bret. Thank you.
Drew:
Thanks for having me, Bret. It’s great to be here.
Listen, Watch & Subscribe on:


Youth mental health refers to the emotional, psychological, and cognitive well-being of children, adolescents, and young adults. This period of life is marked by rapid brain development and…
Read more

The promise of ketogenic therapy for treating mental illness is accelerating with the newly published findings of a pilot study at The Ohio State University, which showed remarkable…
Learn more
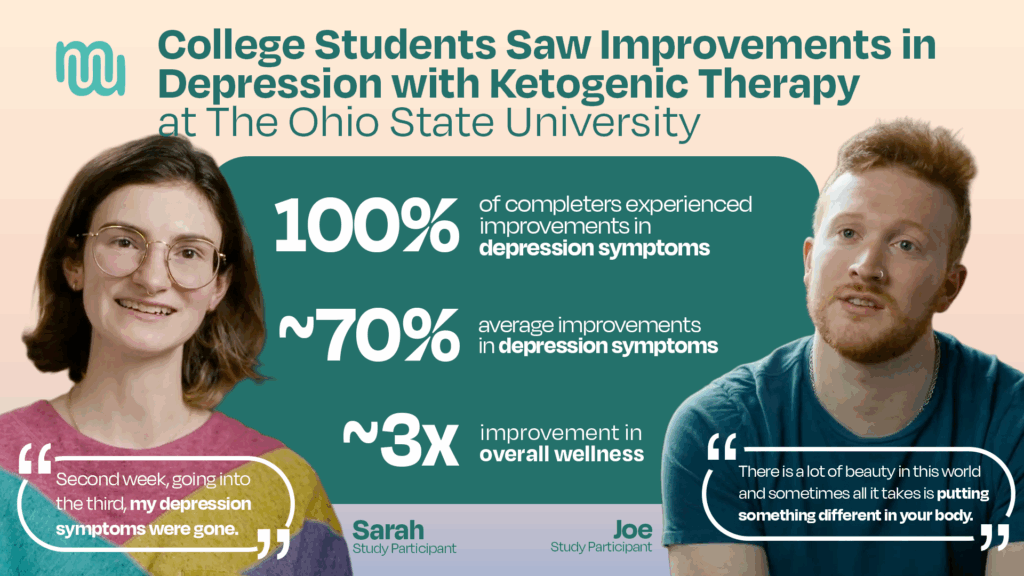
A new study shows an association between at least 10 weeks of following a well-formulated ketogenic diet and a roughly 70% decrease in depression symptoms among a small…
Learn more
ACCORD is proud to announce that the Baszucki Group has awarded more than $600,000 in research funding to support a groundbreaking study on metabolic psychiatry in partnership with…
Learn more
Youth mental health refers to the emotional, psychological, and cognitive well-being of children, adolescents, and young adults. This period of life is marked by rapid brain development and…
Read more
The promise of ketogenic therapy for treating mental illness is accelerating with the newly published findings of a pilot study at The Ohio State University, which showed remarkable…
Learn more
A new study shows an association between at least 10 weeks of following a well-formulated ketogenic diet and a roughly 70% decrease in depression symptoms among a small…
Learn more
ACCORD is proud to announce that the Baszucki Group has awarded more than $600,000 in research funding to support a groundbreaking study on metabolic psychiatry in partnership with…
Learn more