Get the latest on metabolic psychiatry. Subscribe.

Listen, Watch & Subscribe on:



Can Ketogenic Therapy Put OCD Into Remission?
Listen
About the host

About the guest

About the guest

About the host
About the guest
About the guest

Chris:
Going from disabled, from your mental illness, to thriving in life again, to feeling like I am a fully functioning, passionate, energized, human being.
Bret:
Welcome to The Metabolic Mind Podcast. I’m your host, Dr. Bret Scher. Metabolic Mind is a nonprofit initiative of Baszucki Group, where we’re providing information about the intersection of metabolic health and mental health and metabolic therapies such as nutritional ketosis as therapies for mental illness.
Thank you for joining us. Although our podcast is for informational purposes only and we aren’t giving medical advice, we hope you will learn from our content and it will help facilitate discussions with your healthcare providers to see if you could benefit from exploring the connection between metabolic and mental health.
Can ketogenic therapy help improve or even put into remission obsessive-compulsive disorder? There’s not a lot of research on this, but now there’s a published three case series, and I’m joined by Dr. Chris Palmer and his research assistant Aaron MacDonald, to talk about these individuals and the dramatic stories that they shared about their OCD symptoms, debilitating OCD symptoms, that resolved with ketogenic therapy.
So let’s get into the interview.
All right, Chris Palmer, Aaron MacDonald, thank you so much for joining me on Metabolic Mind.
Chris:
Thank you for inviting us. Thank you so much.
Bret:
Yeah, it’s, a pleasure. I’m really excited to talk about this case series that you published about ketogenic interventions, metabolic therapies for OCD, which I think is so important because at Metabolic Mind, we get a lot of comments about what about OCD, has it been studied? And I guess it hasn’t been studied all that much, but you have one of the first publications talking about it. So I definitely want to get into all those details. But before we get too far ahead of ourselves, i’m sure most people know who you are, Chris, but let’s just start with a quick intro.
Tell us who you are in case people don’t know.
Chris:
So my name’s Chris Palmer. I’m a psychiatrist at McLean Hospital, Harvard Medical School. I’ve been here for almost 30 years, and I have been doing work with ketogenic diets for people with severe treatment-resistant mental disorders for over probably 20, 25 years now.
And then wrote a book a couple years ago, called Brain Energy, that proposes the metabolic theory of mental illness.
Bret:
Very good. And for anybody who’s not familiar with Chris, we have, I don’t know, two or three or four other interviews with you on our website and our YouTube channel. So I encourage people to check those out.
But, Aaron, first-time visitor. So thank you for joining us and tell us about yourself.
Aaron:
Absolutely. My name’s Aaron. I am a member of the Metabolic and Mental Health Program here at McLean. I’m also a member of the Brain Energy Team. I recently graduated from Clemson University studying biological sciences. And yeah, I’m here with, studying with Dr. Palmer at McLean, learning about all of what he’s got going on and, working with all the research and all of his brain energy shenanigans.
Bret:
Very good.
Chris:
Shenanigans is right.
Bret:
But very helpful and clinically impactful shenanigans. So, Chris, you mentioned you treat people with serious mental illness and there’s a lot of talk about bipolar disorder, about schizophrenia, about major depression.
There’s now research on that and there’s so many case reports and clinical experience. But there’s less, a lot less, about things that are, don’t fit under this serious mental illness. And, that’s a term every time I use, I say, look, it doesn’t mean that someone’s symptoms and diagnosis isn’t serious.
That’s just the medical definition of it, and OCD is one of those. So, I just want to throw it out there to both of you. Why OCD? Why did you decide to write this case series about obsessive-compulsive disorder?
Chris:
I’ll at least take a stab at a start, and part of it is, I think, commenting on what you just said. I think a lot of people do have a perception that OCD isn’t necessarily as serious as schizophrenia, for example. And for many people, that is absolutely true on both sides of the fence. Schizophrenia can be a devastating, debilitating disorder for more than half of the people who have that diagnosis.
But that doesn’t mean you can’t have schizophrenia, and be thriving actually, and be living a reasonably good life. And people with OCD can have milder symptoms, subtle symptoms, that fall under the radar, as our case series ignored with at least one or two of the people. OCD can actually be a severe, sometimes life-threatening, mental disorder.
It can incapacitate people, and at McLean Hospital, we actually have one of the world’s very few OCD institutes where it’s a residential treatment program where we treat people who have had years, sometimes decades, of medications, psychotherapies and other treatments, and nothing is working for them.
And they can literally be home bound because they can’t get out of their own way. They are just consumed with obsessions and compulsions. And I can say firsthand, even at our premier institute that specializes in severe treatment-resistant OCD, we don’t always get those people better. Even with the evidence-based gold standard treatments of medications and exposure and response prevention treatment and other treatments, not everybody responds.
And so we desperately need better treatments, new treatments. And I think as you’ll, as I’ve actually shared on some podcasts, I myself have suffered from OCD. I had it as a child and I received treatment for it. And the treatment kind of sort of of helped but not tremendously. And so I really do know what it’s like, and I think that ketogenic therapies for some people can be life changing And it really is time that we bring this information out to the world and hopefully stimulate interest in randomized controlled trials.
Bret:
Yeah. How about you, Aaron? What motivated you to look into this?
Aaron:
When I first was onboarded at the metabolic and mental health program, Chris had pitched it to me because of a similar story that I had shared with him. I also grew up with OCD and traditional treatments weren’t as effective for me.
Things like SSRIs and cognitive behavioral therapies helped, but did not address the root cause of my mental illness. And when he pitched the idea, I was very eager to get started, and I’m just very glad that how it went. I’m glad it’s successful, it’s doing pretty well and getting the attention of a lot of people, and like Dr. Palmer said, I hope it gets the attention of scientists and people, who can expand on this research and provide it, high-quality research to those who really need it.
Bret:
Yeah, thank you both for sharing your personal experiences and I think that’s so impactful. You both know what it’s like to go through with this, and you both know the potential benefits and pitfalls of the treatment and how so much more is needed.
So, your motivation is clear. And Chris also for you as a treating psychiatrist, to see so many patients not getting better when you know there’s a potential other intervention. And so you hinted at, hopefully, this will spur randomized controlled trials. So right away we have to say this was not a formal trial. This was not a randomized controlled trial, but tell us how did you select the individuals? How did you collect the data? Aaron, why don’t you start and tell us a little bit about that.
Aaron:
So, the cases were found, the patients were found on with a combination of professional and personal connections.
One of them was found through her advocacy online. Another one was outspoken on social media. The third was, Dr. Palmer, had knew of him through his own private practice. And so we had decided before doing the study that we were going to do three case studies, and that these three were going to be our patients.
And so we were just going to be as honest as possible. Say, let’s just put their experiences exactly as they were. We’re not going to pick and choose people based on who we think has the most exemplar story, that the ketogenic diet fixed all of their problems, nd be realistic. And yes, that was, that was our approach.
Bret:
Very good. Yeah, and so, Chris, right away before we get into the specifics, people will always push back and say, ah, it’s three patients. What does it really tell us? it doesn’t say much, but how do you interpret that? How do you respond to that?
Chris:
I can make arguments on both sides of the fence and in support of the case series.
These are people who suffered from OCD for years before they found effective relief. All three of them, independent of each other. We did not introduce them to each other. We did not share their stories with each other. They all independently reported to us that their symptoms improved dramatically when they were on ketogenic diets.
When they went off of diets, when they went off of the ketogenic diet, most of them, or all of them, actually had a return of symptoms. And then when they went back on ketogenic diets, their symptoms again improved. And so, in that way, we are not at all proposing that the ketogenic diet cured their OCD because if it cured their OCD, they would be able to go off the diet and be free of OCD. A cure is like an antibiotic where you take it for a short period of time and then you don’t need treatment anymore. You go on your merry way. And these three individuals have strongly suggested that they continue to need the intervention.
They continue to need to follow the diet in order to have symptom relief. But that is a powerful kind of AB/BA kind of a pattern in which, we see that when the treatment is on, we get symptom relief. When the treatment is off, it doesn’t. Now, some of the pushback will include things like these are three patients for whom it clearly worked. Because there may be hundreds or thousands of people who tried a ketogenic diet, it did not improve their OCD, and they’re not sharing that story. They’re not passionate about getting that out there.
And that’s why I suggested earlier, I’m hopeful that it will spur randomized controlled trials where we can see for sure how many people does this work for, and how many people doesn’t it work for. At the end of the day, though, there’s a tremendous amount of basic science research on brain energy metabolism, on neurotransmitters, on the impact of ketogenic therapies, to know both from basic science and from animal models, that we need to take this seriously. That this is a real potential treatment.
Bret:
Yeah. I really like how you said that, Chris. That was very well said. And when the research isn’t being done, you need to start somewhere to spur the interest of that research. And you hinted at mechanisms, which I want to, or potential mechanisms, which I want to get to in a minute.
But first, Aaron, I want to talk about these case, these or these individuals. They aren’t case series, they’re individuals. They’re people who are truly suffering. If you read the stories, the first patient sounds like symptoms started at age four. And he had lived with it, or he or she, I’m not sure, I lived with it for most of their lives until, interestingly, reducing grains seemed to help. But it wasn’t until that next step of actually being in ketosis that this individual found cessation within two weeks. So, I’m curious if that struck you, about it almost seems like a stepwise approach.
That dietary approach helped, but it wasn’t until the person was in ketosis to really have cessation of symptoms. Is that, sort of how you saw that too?
Aaron:
That’s right. So, he struggled with some weight problems in his youth. And through pure serendipity, his parents found that cutting grains, while also helping his weight issues, and cutting sugars and other carbohydrates, they also helped with his mental health symptoms.
He was able to focus better. His anxiety was down, and his OCD symptoms also decreased. And so his OCD symptoms, at one point when he was about 16, his OCD symptoms came back while he was on vacation. As someone who stays on a low carb regimen himself, when you go on vacation, you don’t want to stay on a low carb diet.
You want to enjoy all the, you go to Hawaii, you want to eat all the fruits and vegetables, maybe you have a drink or two. And so he found himself in this position and while he was in his hotel after feasting on some high carbohydrate meals, he found himself obsessing over the shampoo bottles and conditioner bottles in his hotel room. And he stayed up late into the night organizing them and ruminating about them and couldn’t go to sleep until it felt just right.
And as Dr. Palmer alluded to, OCD can be debilitating for a lot of people. Incredibly invasive and pervasive in people’s lives. When he started to implement the diet again, these symptoms went away, which again shows us that there may be something going on here with ketones and with fat metabolism.
With all the mechanisms we’re going to delve into.
Bret:
Yeah, I mean that it’s a striking example, and which actually leads me to the second case study, which I don’t know, you could say is an even more striking example because the quote that just jumped off the page to me was the second individual said they thought the only way out of their OCD symptoms was death.
Like they truly thought that was the only way out at one point in their lives. And yet, here they are, two weeks after being in ketosis with resolution of their symptoms. That really struck me as it doesn’t get any more dramatic than that. So what was your interaction with this individual and your take?
Aaron:
She had particularly, for me, disturbing obsessions. Hers were characterized by these violent, intrusive thoughts to harm her family, to harm her roommates in college. And it affected her ability to connect with the community around her, with her loved ones and her support network, and so she wasn’t able to enjoy being with family.
She wasn’t able to enjoy making friends at college. Something that is an experience for all of us. When we go to college, we meet new friends, we start a new exciting life in a way, and her OCD symptoms tormented her so much that she would walk around in the middle of the night on campus to avoid the people that she cared about out of fear that she would harm them.
She disposed of any objects in that were at her disposal that could be used to harm her friends and family. And she eventually dropped out of college to take some time to address these symptoms. And after some conventional treatments, some therapies and things, she found some relief and was able to continue college as many people with OCD can.
However, when she later moved in with her partner, certain things came about that stressed her, and the OCD came back to full force, as I believe she said it. At the same time, she noticed some weird discolorations, I don’t know if it was some bruising or what it would’ve been, on her abdomen while she was showering and she decided to go on a ketogenic diet for weight loss, much like case one. And out of pure animosity found that the ketogenic diet seemed to decrease her symptoms of OCD rather quickly for her for within two weeks.
Bret:
Yeah, that’s so dramatic. Chris, let me turn to you for a second. In both of those first two cases, symptoms resolved or improved dramatically within two weeks, which seems pretty dramatic. What do you think about that timeframe of action?
Chris:
Honestly, I am, I was and am a little surprised that it happened that fast for them.
What I have found in my clinical work is that even with other patients, and one of these people has been in my clinical practice, what I have found with a lot of people is that they almost always get mood improvement within two weeks. And that can be profound for somebody who is debilitated by a mental health condition, whether it’s OCD or schizophrenia or bipolar or whatever.
And so I think to some people it can feel like, oh, this weight is being lifted off my shoulders. But what I’ve also found in particular with chronic psychosis and with OCD in other patients is that those types of symptoms can take many weeks, if not months, to fully resolve. That they’re saying, I feel so much better, but as a psychiatrist I’m pushing them, but what about those thoughts?
What about those delusions? What about the hallucinations? And sure enough, they’re usually still there. And so one of the reasons I really want to highlight this is because I’m worried that some people will hear, oh, two weeks, and it should be all better. And then they’re going to prematurely abandon an attempt at therapeutic ketogenic diet for their mental illness thinking that it didn’t work for me in two weeks. So it must not, it won’t work for me. And I don’t want anyone to come away from these particular cases thinking that is the way it works for everybody.
Because as a clinician, I’m here to tell you that’s not the way it works for everybody. For some people, it can take three months, four months to really see significant improvement in the symptoms. Again, usually we’re seeing some signal at two weeks, but it may not be the life-changing remission of illness or symptoms that you’re looking for. And I would just encourage people not to give up yet.
Bret:
Yeah, such an important point to get that clinical experience and understand the timeframe is different for everybody, and which leads to the third case, which is an individual who’s an individual who did have a more prolonged course of symptoms even on the ketogenic diet. It sounds and it took maybe up to a year before seeing a resolution of symptoms.
So how does that case compare and contrast to the others, Aaron?
Aaron:
Case three was an interesting individual. She is what I would consider much more treatment-resistant. She tried conventional treatment. She went to therapy. She did cognitive behavioral therapy. She took SSRIs and atypical anti-psychotics to treat her OCD, but the problem she faced was the side effects of some of these anti-psychotics.
She would find herself sleeping for most hours of the day, and she would only wake up to take her children to school. And then would come home and sleep again after already having a full night’s rest. And so she would probably sleep between 16, 20 hours a day, and so she was less plagued by her OCD and other mental health conditions, but her quality of life was horrible.
No one wants to spend their whole life asleep and doing nothing and unconscious. People want to feel alive. They want to have energy. They want to feel passionate about things and enthusiastic about things. The ketogenic diet has side effects that don’t include pervasive sleepiness, like some atypical antipsychotics.
So, the ketogenic diet can help people lose weight, they can help, it can help mitigate cardiovascular disease risk. The ketogenic diet helps people feel excited about life again.
Bret:
Yeah. So it, when someone’s on a keto diet, and if they’re losing weight, if they’re having more energy and if they’re able to reduce the side effects of their medications, that alone can just change their whole outlook on life.
And that’s clearly very dramatic. Chris, tell us about your experience with people who are, we can use this one case in the broader perspective, of people who are experiencing side effects of their medications that are so profound. Like Aaron just relayed about this one individual and then using ketogenic therapies and metabolic therapies, how do, in your experience, how does that help people with those side effects or with the medications?
Chris:
Yeah, I think for some people it is nothing short of miraculous. And again, this is not across the board. Not everybody’s going to get this miracle response, but it’s also important that we do share with the world that this can happen, and that this is happening for people.
And what I’ve seen is, in particular for people with treatment-resistant mental illness, and for the most part, those are a lot of the people who are trying the ketogenic diet because if they’ve tried a pill, and it worked beautifully and it came with no side effects, they’re just living there happy ever af after life.
And they’re not really usually going out trying a ketogenic diet to see if they can replace their medications. But for the millions and millions of people for whom medications are not fully working and or come with burdensome side effects, when you can do a treatment that not only alleviates your suffering, that not only gives you more in energy, that not only helps you feel like your brain is firing on all cylinders for the first-time in years or decades, but now you don’t have to put up with these burdensome side effects.
That yeah, I think it can be going from disabled from your mental illness to thriving in life again. To feeling like I am a fully functioning, passionate, energized human being, and I can do things. I can do the things that I want to do. I can put my mind to things and get them done.
And I just want to point out one, the first case in our series is a Harvard College student and, who did spectacularly well on SATs and school, and is doing great at one of the most elite colleges in the world. And it’s important to note that because he had a mental health condition and these usually slow people down, the side effects slow people down.
The symptoms slow people down. They reduce self-esteem. They can impair cognition, they can impair motivation, and he is thriving. And I think that, and the others are thriving as well, and I think it’s just important to note that.
Bret:
Yeah, such a powerful example of how people can live with and live beyond these diagnoses.
That they have, and just as an aside, we have so much content about managing medications, about tapering and with the key message being that people should not be doing this on their own. They should be doing it in conjunction with their prescribing physician because so many different things can happen. But I think it’s becoming clear that with metabolic therapies and ketogenic therapies, it can open a door for potential safe tapering and deprescription when with your prescribing physician. I know you feel strongly about that as well, Chris, and I don’t mean to go off completely on that tangent, but I just want you to be able to emphasize that point as well.
Chris:
No, I, agree, and I appreciate that. And I think it is important.
People understand that changing medications is can be very challenging, and sometimes dangerous, and that they should not try to change their medications, especially going off of them on their own. That they should just do that with the help and supervision of a medical professional who knows how to do that safely.
Some medical professionals don’t even know how to do that safely. So find somebody who knows what they’re doing, and do it well so that you can stay out of trouble.
Bret:
Very good. Aaron gave us a very good detailed analysis of these three individuals and their dramatic changes that they saw. Now, why does this work? We’ve heard explanations about in when if someone has bipolar disorder or if they have schizophrenia, Chris, the way your book explains it, an altercation in the brain energy and the way that the brain can transform energy. It’s disruptive and that can lead to various symptoms.
So, how can that lead to symptoms of a bipolar disorder or symptoms of OCD? Like how can one mechanism potentially lead to completely different symptoms?
Chris:
So, I think it, the first thing to say is that metabolism is ridiculously complicated. it’s not one mechanism. It’s actually hundreds, if not thousands, of enzymes and pathways and other things that can go wrong.
But at the end of the day, thinking about it in terms of metabolic terms is actually extraordinarily helpful because some therapies enhance metabolism and other therapies can actually impair metabolism, and that is really important to know. And so I would say first it’s not one mechanism. It’s many mechanisms.
And so one could surmise that somebody might have vitamin B12 deficiency, for example, and that can impair mitochondrial function, brain energy, metabolism. And that might result in one constellation of symptoms for one individual. Somebody else might have insulin resistance due to a really poor diet, high-end ultra-processed foods. And that might result in a different constellation of symptoms that include maybe metabolic health issues like weight or pre-diabetes, but also mental health conditions like depression, anxiety, or even OCD or even bipolar or schizophrenia.
So why differences in different people? Because metabolism is so complex. That means there are many different ways that it can go wrong. And depending on which brain regions are impacted, you’re going to see different symptoms. Just like somebody can have metabolic syndrome, so somebody can have poor metabolic health.
One of those people might have high blood pressure and pre-diabetes, and another person may have perfectly normal blood pressure but have type two diabetes out of control. And I could go on with different permutations. And so how does that make sense? Like one person’s blood pressure’s fine, the other person’s not, one person only has pre-diabetes, the other has severe type two diabetes.
Is there anything in common with them? Yeah, there’s a lot in common with them. They have poor metabolic health, and at the end of the day, a low carbohydrate diet might help all of them, regardless of which ones you have. And so a similar thing can happen in the brain depending on which brain regions are impacted.
One person might have OCD, another might have schizophrenia, another might have bipolar symptoms, and yet metabolic therapies can sometimes help any or all of them. And it’s just really important to point this out. This seems like a little challenging to believe for some people. There’s a fine line between schizophrenia and OCD.
A lot of people who have schizophrenia also have OCD. Some of the treatments that we offer, for example, Zyprexa or Olanzapine, is known about 30 to 40% of people with who are taking Zyprexa and Olanzapine can end up developing OCD symptoms. And it’s a side effect of some of our treatments that are harming metabolism that cause weight gain, that cause type two diabetes, that increase risk for cardiovascular disease.
Oh, that also cause new mental health conditions. And I guess what I’m saying is it’s all interconnected. And although it’s complicated, it is understandable, and we can do better.
Bret:
Yeah. And it’s important to note how there is so much overlap between these diagnoses. And you’re given the diagnosis that maybe is the predominant symptom to fit with the, the DSM-5 criteria, but that doesn’t mean that’s your only symptom.
And, that there is such an overlap and comorbidity between all these diagnoses that they often coexist. Yeah, so Aaron, did you see that in the individuals, too? That it wasn’t just clear OCD and that’s it? That they had other symptoms that could be given other diagnoses maybe if the OCD wasn’t the prominent diagnoses?
Aaron:
Oh, absolutely. Some of the patients did, in fact, have other diagnosed mental illnesses. Case three was diagnosed with bipolar and also suffered from postpartum depression. Case one had generalized anxiety disorder. And it just goes to show that in mental health research, we need to start looking for transdiagnostic indicators.
Many mental health disorders are associated with metabolic dysfunctions. And so if these, if the metabolic dysfunction is at the root of these mental health disorders, then metabolic therapies can be used to treat mental illness.
Bret:
Yeah, that’s a very good point. Yeah. Now, to wrap us up here. Chris, you had mentioned you hope this will inspire future studies in randomized controlled trials to look deeper into this, and I certainly hope you’re right.
But that’s going to take years probably before we get a published paper. So between now and then, what should a clinician do? A clinician who is sitting across from a patient experiencing OCD that’s impacting their life. Should they all be talking about ketogenic therapy?
Chris:
I think that ketogenic therapy should be on the menu of options. In particular, if patients have exhausted many of the evidence-based treatment strategies. So, if somebody has already been on three or more antidepressants, serotonergic, antidepressants at high doses, and those haven’t worked. And they’ve augmented with atypical antipsychotics or they’ve had trials of exposure and response prevention treatment. So, these are some of the more usual evidence-based treatments for OCD. And the two strongest ones are exposure and response prevention, which is a cognitive behavioral therapy or SSRIs or serotonergic antidepressants. Those are the two mainstays.
I can’t tell you how many people, millions of people, are still suffering from OCD and they’ve tried those things. Or if they haven’t tried exposure and response prevention fully, it’s because they got overwhelmed with fear and anxiety. When a therapist even mentioned it or tried to get them to do it, they became incapacitated with anxiety. And they couldn’t follow through with the treatment.
And I, so I think for those patients, and maybe for patients who just want to avoid medications or want to try something different, it is not unreasonable to at least consider the ketogenic diet. Because again, there are a lot of mechanisms of action that help us understand how and why this would work for OCD.
And now we’ve got some published case studies to document that for some people, this actually can work and can be life changing and can be sustainable for years, and was an effective enough treatment and an easy enough treatment that they all came back to it again. All three of them at some point or another, tried to go off the diet or veer off the diet or do something different with the diet for good reason.
As Aaron was saying, if you’re on vacation in Hawaii, sure have some pineapple, have a cocktail or something with a lot of fruit in it because that’s what people do when they go to Hawaii. So who doesn’t want to do that? And yet if that, if doing that torments you, if that makes your OCD come back with a vengeance and now you’re stuck in your hotel room crippled by OCD. There’s nothing fun about that. It’s no longer a vacation. And now you’re just in a living hell. And so doing the diet is a piece of cake. Pun, I guess intended, doing the diet is a piece of cake compared to having crippling OCD. Yeah.
Bret:
Yeah. Very good. I want to thank you both for joining me today and for your work. For taking the time to write up this case series and publish it.
Because like we’ve talked about, this is an area that needs so much more work and so much more understanding, and this is definitely the first step. So thank you very much. And, actually Chris, before we go, just let everybody know where they can follow you because you are very active on so many different arenas.
Chris:
Yeah, people can, I’ve got a couple of websites, brainenergy.com, chrispalmermd.com focused on slightly different things. Chris Palmer, MD’s focused more on some of my academic work and some of the research papers and other things, but people can find me on X, Chris Palmer, md. They can find me on Instagram, Facebook, LinkedIn, all sorts of places.
Bret:
All right. And then Aaron, before we go, how about you? Where can people find you?
Aaron:
You can find me on X @MetabolicMac.
Bret:
Metabolic Mac like that.
Aaron:
Yep. You won’t find me on mu much other platforms because I try to minimize that stuff.
Bret:
All right. Very good. Thank you both so much, and I look forward to seeing more from you in the future.
Aaron:
Thank you, Bret.
Chris:
Thanks so much.
Bret:
I want to take a brief moment to let our practitioners know about a couple of fantastic free CME courses developed in partnership with Baszucki Group by Dr. Georgia Ede and Dr. Chris Palmer.
Both of these free CME sessions provide excellent insight on incorporating metabolic therapies for mental illness into your practice. They’re approved for a MA category one credits, CNE, nursing credit hours, and continuing education credits for psychologists, and they’re completely free of charge. On mycme.com. There’s a link in the description.
I highly recommend you check them both out. Thanks for listening to the Metabolic Mind Podcast. If you found this episode helpful, please leave a rating and comment as we’d love to hear from you. And please click the subscribe button so you won’t miss any of our future episodes. And you can see full video episodes on our YouTube page at Metabolic Mind.
Lastly, if you know someone who may benefit from this information, please share it as our goal is to spread this information to help as many people as possible. Thanks again for listening, and we’ll see you here next time at the. Metabolic Mind Podcast.
Listen, Watch & Subscribe on:

Could nutritional ketosis unlock therapeutic breakthroughs in treatment-resistant obsessive-compulsive disorder (OCD)? A newly published, peer-reviewed case report in Frontiers in Psychiatry unveils a potential missing link in the…
Read more
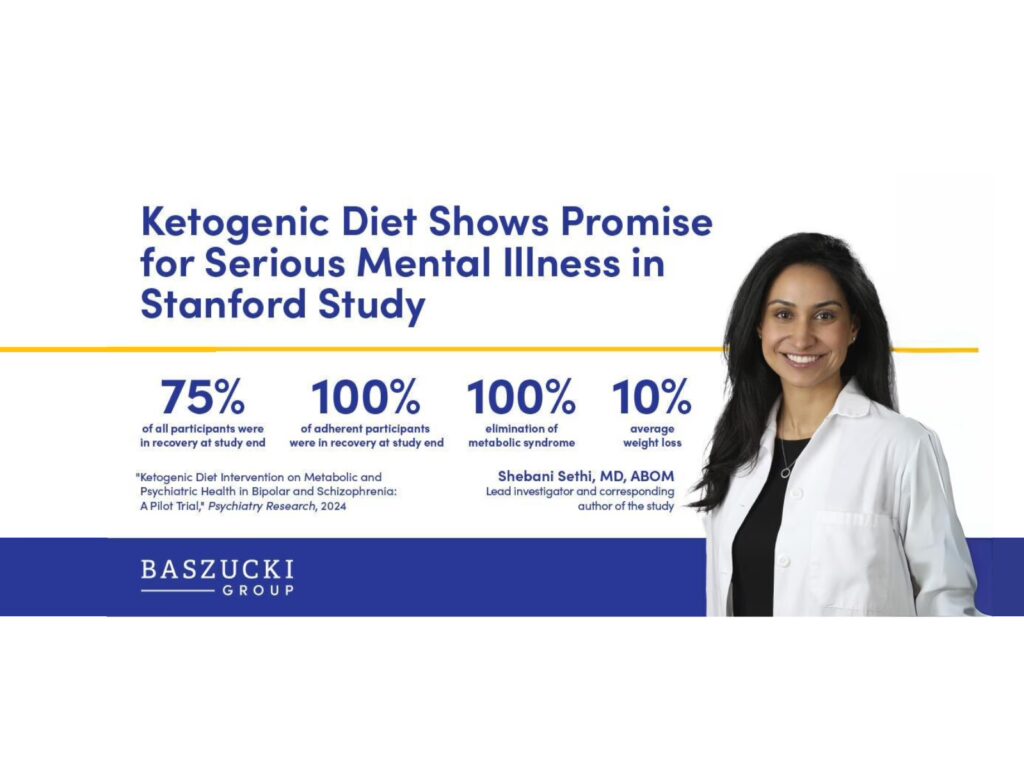
Peer-reviewed clinical pilot trial reports dramatic improvements in psychiatric and metabolic outcomes in bipolar disorder and schizophrenia
Learn more
Harvard psychiatrist Dr. Chris Palmer outlines a new understanding that unites our existing knowledge about mental illness within a single framework.
Learn more
What’s the difference between a low-carb diet and a ketogenic diet, especially when it comes to mental health? In this premiere Mailbag episode, Dr. Bret Scher (Medical Director at Metabolic Mind) and Harvard trained psychiatrist Dr. Georgia Ede answer some of the most common questions they receive about ketogenic diets specifically for mental illness.
Learn more
Could nutritional ketosis unlock therapeutic breakthroughs in treatment-resistant obsessive-compulsive disorder (OCD)? A newly published, peer-reviewed case report in Frontiers in Psychiatry unveils a potential missing link in the…
Read more
Peer-reviewed clinical pilot trial reports dramatic improvements in psychiatric and metabolic outcomes in bipolar disorder and schizophrenia
Learn more
Harvard psychiatrist Dr. Chris Palmer outlines a new understanding that unites our existing knowledge about mental illness within a single framework.
Learn more
What’s the difference between a low-carb diet and a ketogenic diet, especially when it comes to mental health? In this premiere Mailbag episode, Dr. Bret Scher (Medical Director at Metabolic Mind) and Harvard trained psychiatrist Dr. Georgia Ede answer some of the most common questions they receive about ketogenic diets specifically for mental illness.
Learn more