Get the latest on metabolic psychiatry. Subscribe.

Listen, Watch & Subscribe on:



Keto, Microbiome, and Depression: A New RCT led by Dr. Timur Liwinski
Listen
About the host

About the guest


Timur:
I guess it’s not a secret that treatments basically for all mental conditions aren’t working optimally, but especially, in depression. I think that effective biological treatments, they remain elusive. But there seems to be like an overall one pretty stable, species adequate diet for each and every species, and animals are the healthiest if they stick to it with minor variation.
Bret:
Welcome to the Metabolic Mind Podcast. I’m your host, Dr. Bret Scher. Metabolic Mind is a nonprofit initiative of Baszucki Group where we’re providing information about the intersection of metabolic health and mental health and metabolic therapies, such as nutritional ketosis as therapies for mental illness.
Thank you for joining us. Although our podcast is for informational purposes only and we aren’t giving medical advice, we hope you will learn from our content and it will help facilitate discussions with your healthcare providers to see if you could benefit from exploring the connection between metabolic and mental health.
Dr. Timur Liwinski is a clinician scientist in Switzerland, trained in internal medicine, metabolic health and an expert in microbiome research and now is in his psychiatry residency. So, he’s perfectly positioned for his role in nutritional and metabolic psychiatry, and he’s launching a ketogenic diet for depression study.
So, we talk about his study and a lot about the microbiome, what we know and what we don’t know, and ketogenic diet’s impact on the microbiome. So, stay tuned for the interview.
Dr. Timur Liwinski, thank you so much for joining me today at Metabolic Mind.
Timur:
Hi, Bret. Thanks for having me.
Bret:
Yeah, I was really excited to learn about your trial that you’re doing for a ketogenic intervention to treat depression. So, I thought what a great opportunity to learn more about you and your journey, how you got into metabolic psychiatry and hear about this trial that you’re doing.
So, why don’t we just start from the beginning? You have an interesting story that you’re both an internist, you went through residency in internal medicine, and now you’re in residency in psychiatry. So, tell us a little bit about your medical journey.
Timur:
Yeah, so my medical journey hasn’t been quite linear.
I studied medicine in Germany, and I was actually, like towards the end of med school, I was really interested in psychiatry. And I’ve also pursued actually my doctoral degree in child psychiatry. And I guess at that time, I got somewhat disillusioned with the treatment opportunities that we had back then, and which are basically also unchanged now almost 10 years after I finished my doctoral degree.
And I somehow had the idea that I have to pursue like somatic medicine because I really want to make an impact, and basically, help and heal every patient. And like after a stint in neurology, I pursued residency in internal medicine with a focus on gastroenterology, but also endocrinology, metabolism, and also nutritional medicine.
And after a few years, I actually realized that even in internal medicine, we are mostly treating symptoms, and in many cases, far too many, we aren’t even successful with that. And so I guess, naturally, that reignited my interest in research. So, I really wanted to basically break the disease code and help in developing new therapies.
And that was back in 2016, 17. And as a gastroenterologist, the hottest thing was, of course, microbiome research, and this is what I pursued. At that time, I took a complete break of clinical work and I started my first postdoc that with Stefan Bonn in Hamburg at the Institute for Medical Systems Biology.
And I studied the interaction between the microbiome, immunity and diet in autoimmune liver diseases, especially PSC, which is a detrimental autoimmune inflammation of the bile ducts, and which is in most cases accompanied also by inflammatory bowel disease. I studied the microbiome in the gut and also the bile ducts and got really intrigued and wanted to take it basically to the next level because my research at that time was more, I studied more correlations and associations rather than causal relationships.
So, I wanted to step up my research, and I applied for a postdoctoral fellowship at the Weizmann Institute of Science with Eran Elinav, who was like really a household name in the world of microbiome research.
And yeah, that was successful. And so I embarked on my second postdoc. And for three years, we studied, basically, in mice and in humans, the microbiome interactions, immune system and diet, of course, in different disease models, different conditions. I worked on the project on Alzheimer’s disease, but also inflammatory bowel disease.
And one thing that was really big at that time and where our lab has like really done cutting edge research is personalized diet, which really intrigued me and got me into this whole like diet and dietary therapy world. I studied that, sounded interesting, like the variation in glycemic responses.
However, I came to the personal conclusion that it’s probably less about fancy personalization, like based on your microbiome parameters and a myriad of predictors. I noticed that actually most people who had more favorable glycemic responses and metabolic parameters after adopting a personalized diet, most of them actually reduced their carbohydrate intake.
And at that time, I still didn’t really discover the ketogenic diet. I heard about it, but for me at that time, like keto was basically inextricably linked with ketoacidosis, which I treated in during my residency in the emergency department, which I, of course, like dreaded. It’s this horrible and dangerous thing.
And it was actually, despite all of the science that I studied at that time, it was actually personal inspiration that made me embark on the keto journey. And my now father-in-law, and I met my now wife at that time, he’s been diagnosed with pre-diabetes. And like he is a really intelligent and curious guy, and somehow, he did his research.
He didn’t just trust his doctor, who, of course, recommended him the standard lose weight, exercise, adopt a hypocaloric, low-fat diet. But he did his research, even though he’s like not from the field of medicine or science whatsoever, and he discovered the ketogenic diet.
And at that time, when I think it wasn’t as widely popular, there weren’t that many resources available online and on social media. He adopted that, implemented it successfully and really restored his health. And that really made me think and made me curious and motivated me to really scientifically, seriously scientifically study the ketogenic diet.
Bret:
Yeah, and then, if you look at it, there was nobody in a better position, better trained than you, as being trained in internal medicine, endocrinology, microbiome, nutrition, like anybody like that should have learned about the ketogenic diet, if it was a fair playing field, so to speak, if people talked about all diets as options and wanted to explore them scientifically.
But I think it shows the bias against ketosis within the medical community that you didn’t learn about it, that it wasn’t taught about, that it wasn’t discussed. And you had to find it in a totally different way, a totally independent way, from your father-in-law, not from all the academic and clinical work you’re doing.
I find that amazing, I mean disheartening, but also just you have to laugh about it in a way. And it’s now because of where you are and because of what we’re doing in so many in this field are doing, hopefully, that’s going to change. But then through this, you found your way to psychiatry. So, now you’re doing a psychiatry residency and with this personal understanding of ketogenic diets and researching it or learning more about it academically.
Now, you’re starting a research study on ketogenic diets for depression. So, tell me how you got to that point of saying, wait a second. Now, here I am in psychiatry. I can see what treatments we have available. I can see where maybe we’re lacking?, And I can see where ketosis might play a role here. So, how did you get to that part?
Timur:
Like you you said it, that now my entire career so far seems to make sense. Like I guess that I didn’t plan it that way, of course, 10 years ago, but probably it’s this.
Human needs to create a coherent live narrative so that drove me. And I must say, I had, how should I say, extra scientific inspirations to return to psychiatry. At that time, I got really serious about mental health and I guess I felt the need to not abandon everything I’ve learned so far, but somehow link it all up together, metabolism, diet, microbiome, mental health.
And then I was searching for ways like how to implement metabolic treatments, how to implement diet in psychiatry. And like at that time, it was In late 2020, early 2021, that was before Christopher Palmer became famous.
But there were already authors, who really studied the ketogenic diet seriously as a potential treatment for mental health. I think that like really serious work in mice dates back the late 19, to the late 200os. And I discovered those papers and also some interesting pilot trials in children with autism spectrum disorder that were published in the early 2010s.
That really inspired me.
Bret:
Yeah. and so now with your study that you’re starting, you’re focusing on a ketogenic diet for depression, right? So, tell us why specifically did you pick depression? Because we’ve seen studies on bipolar disorder and schizophrenia and some that combined, bipolar disorder, schizophrenia, schizoaffective disorder, depression.
So, why did you want to focus specifically on depression?
Timur:
I guess there are many reasons. I think like many people who get invested into health, the science of health and healthcare, I also have a personal story. Certainly, in my life, I had my fair share of depressive episodes. And also it’s simply extremely common and extremely relevant.
I think we all know the predictions that by 2030, if it isn’t already, it will become the leading cause in the world of disease burden and the years left with disability. And I must also say another thing that I noticed during my academic journey, and later it was confirmed by studying the literature, is also the poor mental health and academia.
I’ve seen that a lot in my peers to be honest and, I guess, I also experienced a fair share of that myself. And that got me interested in depression and also the opportunities. I guess it’s also the excellent infrastructure in our center to study specifically that condition, and also the funding source that is supporting our study that has been set up by a philanthropist who has her experience with depression and, specifically, studying depression research.
So, for all those reasons, I decided to focus on depression. And I guess another important reason is that, I guess it’s no a secret that treatments basically for all mental conditions aren’t working optimally but ,especially, in depression.
I think that effective biological treatments, they remain elusive. And I think we know that at least in the acute phase that antidepressants, they probably help way fewer people struggling with depression than, for example, the anti-psychotics help people with acute psychosis or mood stabilizers, like lithium, can help people have bipolar disorder. So. I guess it’s also my personal like perceived lack of an effective biological treatment.
Bret:
Yeah, I think that’s a very good explanation for all the many reasons why someone would pick this.
So, that makes a lot of sense. Now, we talked about how you had to learn about this outside of academia, outside of clinical medicine. So, when you bring it up within academia and clinical medicine that you want to study this, was there any skepticism or pushback or no, ketogenic diets aren’t healthy, we can’t do that?
What kind of response did you get?
Timur:
Actually, I was surprised that I got a really positive response, and that wouldn’t be possible without the director of our clinic, Undine Lang, who was immediately excited and very supportive about my ideas and who is generally really interested and in this new or revitalized maybe rather signs of diet, metabolism, gut brain access and mental health.
And I think most of my colleagues were, are really supportive. It’s really interesting how well received it is by those who actually meet the patients because I think they know best that what we are doing isn’t working well for way too many people. And I think for people who even haven’t studied medicine or science, it’s intuitively clear that there must be some kind of lifestyle or dietary way to effectively treat these conditions.
So, yeah, overall the response was really positive.
Bret:
Yeah, that’s great. That’s great. is this trial going to be in-person? So you have to be local or can people join remotely?
Timur:
Yeah, it’s, so initially you have to join locally and, eventually, people have the option to transition to remote support.
But for insurance reasons, you’ve got to be, you got to be a resident Switzerland.
Bret:
And it’s an eight-week long randomized controlled trial with a ketogenic intervention compared to the guideline-based dietary treatment. Is that right?
Timur:
So, I think it’s a challenge in depression to find the right timeframe that makes it probably different from residual symptoms and schizophrenia or mood stabilizing treatment and bipolar disorder.
And that for most people, lack any episodic disorder. And then within a few weeks or a few months, for most people, basically, their condition gets better, even without treatments, spontaneously or resolves. So, I think the challenge here is to really find like a reasonable treatment interval.
And we have now set on 10 weeks, actually. So, at two weeks, adaptation induction phase, followed by eight-week days where people are supposed to be in state of ketosis.
Bret:
And are you going to provide the meals? Are you gonna have a nutritionist teach them how to prepare the meals? How’s that set up?
Timur:
Yes. We actually have a team of nutritionists with like really amazing expert, Katarzyna Hongler, who has joined our team who is the leader of the ketogenic metabolic therapy. I will also provide some of the education and support because I also got my training with and Beth Zupec-Kania and Denise Potter, who of course are household names in the world of keto.
And we are trying to be inclusive and pragmatic. So, we would include people who are treated on an in-patient basis, but we also want to provide it to outpatients and also people who transition from an initial in-patient treatment to an outpatient treatment. And for our in-patients, we’ll also, basically throughout the time that they will stay with us, provide the meals prepared by our kitchen.
Bret:
And what’s the primary outcome measure you’re using?
Timur:
The primary outcome measure is Hamilton’s Depression Scale, 17 items.
Bret:
Yeah, and that’s the same one used by Dr. Danan in his study that he saw significant improvement. So, it’s good to see consistency in tools that are being used so we can, make comparisons across.
I thought it was really interesting if you compare the improvements in the HAM-D for Dr. Danan study and compare it to a nortriptyline study. It’s the exact same numbers, basically the same degree of improvement, the same benefits only with reduced medications and decreased side effects and improved weight loss.
And so all these other things. So it’ll be interesting if you see something similar to that degree. are you also gonna be checking microbiome changes? I’m curious, with your history of microbiome research.
Timur:
This is maybe, I think among all the keto mental health studies going on right now, probably a unique take. Although I think, I don’t remember which one specifically, I think there is, I discovered another protocal by another group who want to study the microbiome.
But yeah, we are aiming to bring that in, study it, by metagenomic shotgun sequencing and hopefully learn as much as possible from that because there is very little research so far on the microbiome and ketogenic diet. And there is a brilliant short review I discovered, have a really catchy title, Microbiome and Ketogenic Diet: Friends or Foe. And I think we haven’t really figured that out yet, but probably depends very much on the specific composition of the ketogenic diet.
Bret:
Yeah, I’d love to discuss the microbiome even further. But first, where can people go if they want to learn more about your trial or see if they can enroll in it, if they’re local to Switzerland?
Timur:
They can just contact me. They can write me an email.
Bret:
Okay, so we will include your email then in the description. Amazing. So, let’s talk about the microbiome for a second though. So, I’m really curious first about what you said with the personalized nutrition. What you noticed was people were just reducing their carbohydrates and that was giving the benefit.
And it speaks to this whole thing like, do we really need to look at someone’s microbiome, look at someone’s genetics to know that we need to recommend lower carbohydrates, lower ultra-processed foods, more whole foods, right? Do we need that for that recommendation or does it have to be, or can it be more specific than that?
Or is this just a field trying to create itself basically? Does that make sense? What, how do you react to that?
Timur:
Yes, I understand. I think probably the proponents of personalized diets and here I’m kind of basically breaking my former mentor, but I guess it’s natural that the student at a certain point rebels against his former mentor.
I think that the importance of personalization, like even though it has a really positive image and like it sounds really promising, personalization, of course, we have to personalize so many things, and we have to put the person right in the center of attention. But I really think that we should not overstretch it.
Because in terms of metabolic health, and, like here I’m basically repeating what Casey Means said. And, many times on different YouTube channels that us humans, we are the only species who has produced pathologists, who has produced like a hundred different medical disciplines.
And yet, we humans are the only species who’s battling with diabetes, and it’s only getting worse. So, we see that in nature, any other species, like their diets aren’t really personalized, but there seems to be like an overall, like one pretty stable species-adequate diet where each and every species and animals are the healthiest if they stick to it with minor variation.
So, I think there is definitely a place for personalization. But I think the personalization isn’t radically different for each and every person, but there is, so to speak, like a mean, I think that there is basically a standard of macronutrient composition and micronutrient needs that a simply species adequate with very few exceptions for humans. The personalization is basically just a minor variation around the mean.
Bret:
Yeah, so when it comes to a ketogenic diet then, some would say that’s a big variation around the mean because of the reduction in carbohydrates. Other would say it’s not at all and it’s perfectly in line with a species-specific diet.
But how do you see ke ketosis playing into this? Is it part of the species specific diet or is it a more of a specific intervention to change biochemistry and metabolism? How do you see that?
Timur:
Yeah, I guess my official statement would be the latter, but my personal hypothesis, I think we have really reliable arguments for that, although it’s certainly not proven yet. But I believe that spending a great deal of time in ketosis, maybe not all the time, but a great deal is probably species adequate.
Bret:
Yeah, and then you mentioned before how there’s still a lot not known about ketogenic diets, ketogenic interventions and the microbiome. And you can see headlines all the time, keto diet is bad for the microbiome, and it’s some rat study where they fed them crisco oil or something.
It’s not like a true keto diet. So, it does seem like the research is pretty poor, and especially if they say a high fat diet. And it’s really, again, in rodents with a high fat and high sugar diet and not really a keto diet. So what do you think we know about a ketogenic diet and the microbiome?
What do we know and what don’t we know at this point?
Timur:
Yeah, we know very little, but I guess we do know that refined grains, and especially sugar, is detrimental to the microbiome. And this is definitely something if we cut that out from our diets, we do our microbiome a great favor. And I think that, although the carnivore community kind of proves us wrong in that regard, in that I didn’t have the chance to take a look at the microbiomes of those people.
And that would be probably a brilliant idea for a study to recruit a sizeable cohort, like of strict carnivores who have been on the carnivore diet for several months, or ideally several years, and look at their microbiomes and what happens to it. But if we assume that the microbiome is so important, and you know those carnivore people that I met, those people look like athletes and they seem to be in perfect health.
If we believe that the microbiome is so important, I can’t imagine like their microbiome be completely devastated.
Bret:
So going back to this need for fiber, basically that you need fibrous and prebiotic type foods to feed the microbiome but yet, as a carnivore, you don’t eat those. But yet, somehow their mental health can improve. Their autoimmunity can improve, if they have an autoimmune condition will improve.
They can lose weight. They can improve their metabolic health. All these things that would seem contrary to not having the quote unquote “healthy microbiome food”. So there’s clearly something we’re missing. Is that right?
Timur:
Like I would probably, so I know that I’m basically also contradicting the consensus, like among the most established, microbiome scientists. I think everyone right now will tell you that fiber is absolutely essential for the microbiome. You have to feed it, and for that you need fiber and also if you other things.
But it seems to me that our microbiome is an omnivore as well, just like our species and gut bacteria, it seems to me that they must be also able to feed from meat as well.
Bret:
Yeah, do you think the, I don’t know, the strength or the certainty of the comments and the recommendations about the microbiome are far ahead of where the research is? Is that a fair statement to make?
Timur:
I think that’s a fair statement to make, and especially all those commercially available microbiome tests, like the promise of, hey, fix your gut health. I think that basically those commercial tests available right now, they’re probably, most of them are probably useless, and it’s really hard. Like we don’t really know how to interpret one individual microbiome sample.
Bret:
Yeah, and like you said, the recommendations frequently are very similar, depending on the results in terms of how people can improve their diet. So, yeah.
Timur:
You’re right. It’s not really a difference. So, exactly. So, we don’t really know. Okay, you have, your probably deficient in a certain species so you have to eat these particular foods. It always boils down to eat more fiber, cut out the sugar. So, you don’t really need this fancy analysis basically to arrive that recommendation.
Bret:
Yeah, and then there’s this talk about the psychobiome, about the connection between the microbiome and our brain health and psychiatry.
And, I guess it’s probably in the same bucket that it’s pretty in early stages. But how do you see that? Do you think it’s. the microbiome directly influences mood and psychiatric symptoms or do you think it’s the lifestyle actions that change the microbiome that influence it? Can we really tease that out at this point?
Timur:
Yeah, my hypothesis is both. And I think with our current study designs that we have and methods, like certain things are simply inseparable, and we can’t, like right now, we can’t have a double-blind placebo controlled trial in dietary interventions. And we can’t really separate, I think the effects of any lifestyle measure, whether it’s mediated by the microbiome or other systems and parameters in your body.
Who knows, maybe in the future we’ll have some kind of ultra realistic, advanced computational modeling with deep learning that we’ll be able to disentangle those effects? But I think, right now, we won’t really be able to tell. But I think I’m too much also of a clinician to care too much about that.
Like all I really want to see is that people are benefiting, and I’m sure there is a host of factors contributing to that. And if it’s a ketogenic diet, yes, the ketone bodies, that’s for sure. Simply ditching sugar, relying on nutrient-dense whole foods. And maybe also the psychological aspect and probably even the spiritual aspect of following certain dietary regime that you heed, that you think is beneficial because, I’m digressing here a bit, but I guess that humans are, most religions for eons have established like certain dietary rules and regulations like, be it halal in Islam or kosher in Judaism.
And I see that people, religious people who are following the dietary rules of their religions, and they feel like they’re deriving some benefit, like maybe it’s some sort of spiritual purity that they experience, and I think it can really benefit their well-being.
Although, it doesn’t really make nutritionally sense. Like for example of kosher food, you’re cutting out seafood, which basically every nutritionist is telling you should be eating, but still people are benefiting. So, I think like this psychological and yeah, even spiritual aspect is also part of it.
Bret:
Yeah, it’s a really interesting perspective. It’s not just all about the biology, physiology, it’s also about other aspects of community, about what you believe to be beneficial about spirituality, how that all plays in. Yeah, really fascinating.
Timur:
Nutritional counseling, I think can be psychotherapy, to be honest.
And I think this is probably also a renegade view. And it’s interesting, like in the pilot study that Shebani Sethi has now published. So, in the method section, they state explicitly that it was just dietary advice, no other form of psychological support was provided in these counseling sessions.
But I think it’s fair to state that. But there’s probably more to that than meets the eye because we know that in psychotherapy research, I think it has shown very clearly that we tend to overestimate the specific content and techniques that we are talking about or employing that what’s really important next to, of course, the massive expectation effects that people have.
It’s the therapeutic relationship, and I think if you have a dietary counselor whom you meet for, I don’t know, six to 12 sessions, and you establish a really, a great client provider relationship, I think that can be a psychotherapeutic as well.
Bret:
Someone cares about me. Someone’s listening to me, someone’s talking to me and wants my well-being. Yeah, that can go a long way. I think that’s such an interesting perspective. This has been a really fascinating conversation. I’m so glad we had you on to discuss this, not only to hear about your trial that you’re doing, but just your journey and your training. I think is exactly what we need.
Someone who knows about metabolism has been trained in metabolism, knows about the microbiome, knows about nutrition, and now is well on his way to becoming a clinical psychiatrist. So, the clinical care you’re going to provide and the research opportunities you’re going to create, I think are just going to transform this field in amazing ways.
So, thank you for sharing your journey with us, and thank you for all the work you’re doing. And I can’t wait to hear more from you in the future.
Timur:
Thank you so much, Bret. I guess that the bar is now really set high and now I have to deliver. And I also want to, I want to thank you for everything that you do for the amazing educational content that you’re providing and really advancing the field of lifestyle, medicine, metabolic psychiatry.
Thanks a lot and thank you for having me. It was a pleasure.
Bret:
Oh, our pleasure. Thank you.
Thank you for watching and for joining us here at Metabolic Mind. Now, please remember that our channels for informational purposes only, we’re not providing individual or group medical or healthcare advice or establishing a provider patient relationship. Many of the interventions we discussed could be potentially dangerous if done without proper supervision.
So, always consult your healthcare provider before changing your diet or your medications. We also have to recognize that there’s not one universal response to ketosis, and there can be variations in how people respond. Alright, but thank you again for joining us, and we’ll see you here next time at Metabolic Mind.
Thanks for listening to the Metabolic Mind Podcast. If you found this episode helpful, please leave a rating and comment as we’d love to hear from you. And please click the subscribe button so you won’t miss any of our future episodes. And you can see full video episodes on our YouTube page at Metabolic Mind. Lastly, if you know someone who may benefit from this information, please share it as our goal is to spread this information to help as many people as possible. Thanks again for listening, and we’ll see you here next time at The Metabolic Mind Podcast.
Listen, Watch & Subscribe on:

A new study shows an association between at least 10 weeks of following a well-formulated ketogenic diet and a roughly 70% decrease in depression symptoms among a small…
Read more

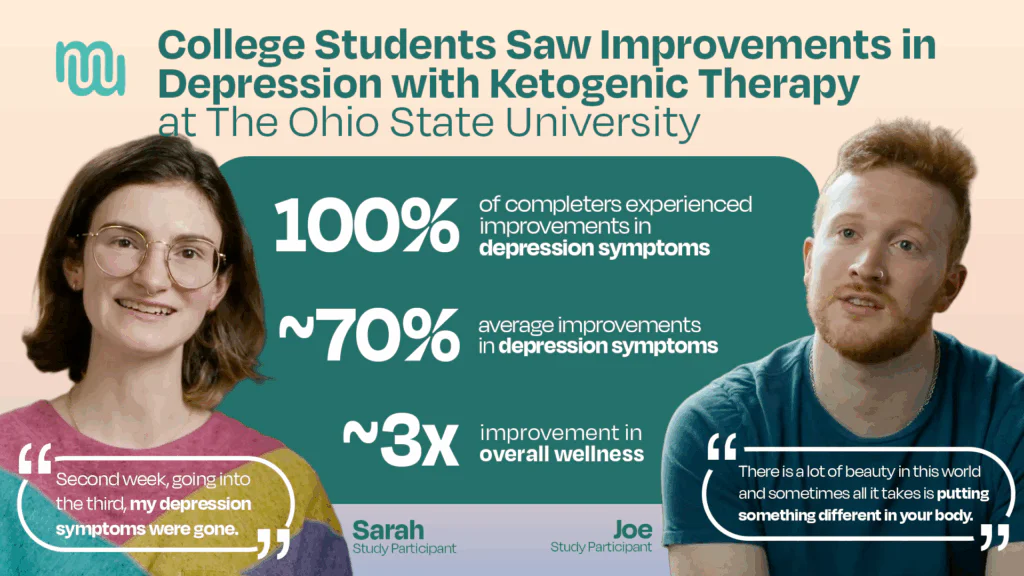
The promise of ketogenic therapy for treating mental illness is accelerating with the newly published findings of a pilot study at The Ohio State University, which showed remarkable…
Learn more
A groundbreaking study from The Ohio State University shows that ketogenic therapy may *dramatically* reduce symptoms of major depression in college students. Dr. Volek has decades of experience conducting research on ketogenic therapy. The Volek Low Carbohydrate Laboratory is one of the best in the game at conducting quality ketogenic science.
Learn more

Deprescribing expert Dr. Mark Horowitz explains why psychiatric-med withdrawal is so often mistaken for relapse, how short-trial guidelines mislead clinicians, and the safer “hyperbolic” taper that uses liquids/compounding to make tiny final cuts. Learn practical signs of withdrawal vs. recurrence, what can buffer symptoms, who should (and shouldn’t) come off, and where to find evidence-based support.
Learn more
A new study shows an association between at least 10 weeks of following a well-formulated ketogenic diet and a roughly 70% decrease in depression symptoms among a small…
Read more
The promise of ketogenic therapy for treating mental illness is accelerating with the newly published findings of a pilot study at The Ohio State University, which showed remarkable…
Learn more
A groundbreaking study from The Ohio State University shows that ketogenic therapy may *dramatically* reduce symptoms of major depression in college students. Dr. Volek has decades of experience conducting research on ketogenic therapy. The Volek Low Carbohydrate Laboratory is one of the best in the game at conducting quality ketogenic science.
Learn more
Deprescribing expert Dr. Mark Horowitz explains why psychiatric-med withdrawal is so often mistaken for relapse, how short-trial guidelines mislead clinicians, and the safer “hyperbolic” taper that uses liquids/compounding to make tiny final cuts. Learn practical signs of withdrawal vs. recurrence, what can buffer symptoms, who should (and shouldn’t) come off, and where to find evidence-based support.
Learn more