Get the latest on metabolic psychiatry. Subscribe.

Listen, Watch & Subscribe on:



Exciting New Research on Keto for Pediatric Mental Health
Listen
About the host

About the guest


Kirk:
I think if we’re able to demonstrate, in fact, that this does demonstrate improvements in metabolic health, improvements in clinical symptomatology, that what that allows us to do is to speak to kind of students who work with youth and say, this should be a tool in your toolbox.
Bret:
Welcome to the Metabolic Mind Podcast. I’m your host, Dr. Bret Scher. Metabolic Mind is a nonprofit initiative of Baszucki Group where we’re providing information about the intersection of metabolic health and mental health and metabolic therapies such as nutritional ketosis as therapies for mental illness.
Thank you for joining us. Although our podcast is for informational purposes only and we aren’t giving medical advice, we hope you will learn from our content and it will help facilitate discussions with your healthcare providers to see if you could benefit from exploring the connection between metabolic and mental health.
Emerging research is telling us a lot about ketogenic interventions for bipolar disorder, but what about in the pediatric population? There are two different studies that are ongoing right now that are probably going to shed a lot of light about using ketogenic intervention specifically for pediatrics.
And given the history of ketogenic interventions for epilepsy, there’s really quite a track record about using it for brain-based disorders. So how’s this going to be different? What’s it going to add to the current framework of using ketogenic interventions? Let’s hear from Dr. Kirk Nylen.
All right, Dr. Kirk Nylen, welcome to Metabolic Mind. Thanks for joining me.
Kirk:
Thanks for having me, Bret.
Bret:
Yeah, it’s a pleasure to interview you always and speak with you. We work together closely at Baszucki Group, but now I get the chance to talk to you about some studies that you’re helping facilitate and, as I’ve talked to you about before, and really appreciate about you, is that you’re really focused on where the gaps in research, where the gaps in science.
And one of them is with with children, with the pediatric population. So we have a couple big efforts to talk about with bipolar in the pediatric population and ketogenic interventions, and I’m really excited to get into. But before we do that, once again, just bring us up to speed your quick background, and then we’ll get into the details.
Kirk:
Sure. So my background, I did my PhD at the University of Toronto in Neuropharmacology. I studied the ketogenic diet and epilepsy. One of the things that we’ll talk about is the irony of the ketogenic diet predominantly being used in a pediatric population, in epilepsy, but we don’t really know the answers to those questions in bipolar.
After completing my PhD, I worked at the Ontario Brain Institute where I led the research informatics programs there, and then had the good fortune of getting to meet Jan at a conference and learning about the work of Baszucki Group.
My interest in ketogenic diet in the different area, and this is, of course, in serious mental illness.
Bret:
Yeah, and I think what’s really germane to this discussion is the sort of the historical knowledge of ketogenic interventions in epilepsy because it’s seen by many as like a quote unquote new interventions. But in the field of psychiatry, and as Dr. Chris Palmer and many others have said, no, it’s not a new intervention because it’s been used for epilepsy for decades, and if not a century, with decades of study behind it.
But the first question is always, is it safe? Okay, we’ll talk about efficacy. We’ll talk about mechanisms. But when you’re talking about an intervention in kids, is it safe? So how do you reflect on that question, and using your experience and your personal experience as well with epilepsy and ketogenic interventions about the safety?
Kirk:
So for me, I ended up starting to study epilepsy just out of a fascination of how neurons worked and how neurons connected to one another and how learning and memory took place.
It became very personal for me. Early in my grad school, my nephew was diagnosed with epilepsy. And despite getting surgery and trying basically all the medications that were available to try, they were not able to control his seizures. At the time, I was working at The Hospital for Sick Children doing research and at the University of Toronto.
And so I was able to help bring my nephew to Sick Kids, where my sister learned how to administer the ketogenic diet for her son, and this was completely revolutionary in his health. They saw immediate effects in the first week, started to see him paying more attention, cognitively being more present.
He was three years old. You notice these things in small children and then his seizures stopped completely. And one of the things that really blew my mind was there was no drug on the market that was able to stop his seizures, but changing his diet could stop his seizures. And the profoundness of that realization that we could be using food as medicine, and that you could think about dialing back the diet or dialing up the diet depending on the need and depending on the condition.
It was really fascinating and it shaped the research work I was doing looking at the effects of the ketogenic diet in epilepsy and how it worked on energy in the brain. So looking at mitochondrial health, and really led to what’s become my full career of looking at how diet could be used to treat different neurological conditions, including psychiatric conditions.
Bret:
Yeah, so from that personal journey, dug in even deeper to the use of ketogenic interventions. And so if someone questions their safety, how do you respond to that?
Kirk:
I think in healthcare, the intervention and the risk associated with it needs to be proportional to the risk of the condition itself.
And I know in kids with epilepsy, the ketogenic diet that’s used is a very restrictive ketogenic diet. It’s four parts fat to one part combined carbohydrate/protein. They often calorie restrict the children so they’re getting their 25% fewer calories than would otherwise be consumed by kids their age, and there’s issues.
The kids don’t grow well. They often have abnormal blood lipid profiles. There are risks associated with it, but the denominator is having a hundred seizures a week. And so in that case, it makes a lot of sense, I think, in serious mental illness, in the space we’re talking about, we’re talking about using a much less restrictive ketogenic diet.
The studies that we support are using a 2 to 1, 2 1/2 to 1 ketogenic diet. You’re not drinking Cupps of oil; you’re having avocado in your salad. So, I think there’s a big difference in when you think about it from a risk profile and a safety profile.
Bret:
Yeah, and I think the amount of protein is a big factor as well because with that traditional 4 to 1 diet, it’s also a very low protein diet. For a growing individual is crucial; you need your protein.
So, this more, or sorry, less restricted, more flexible higher protein ketogenic diet, what I think of is just like the modern keto diet basically. It’s been called modified Adkins in different terms, but it’s really just like the common keto diet now, which is certainly much more sustainable.
So, with that definition, the different definitions and with the background of treating epilepsy. So now, there is a child bipolar network study that you were involved in help facilitate. So tell us about that.
Kirk:
Sure. So this is a study being led out of UCLA by Dr. Miklowitz. and it involves three other sites. So, the child bipolar network includes UCLA, the University of Cincinnati School of Medicine, University of Colorado Medical Campus, and the University of Pittsburgh Medical Center.
So, those four sites are all involved in this randomized control trial. So it’s a randomized control trial, which means there’s two arms and people will be assigned to either the intervention arm, which is the ketogenic diet plus standard of care, or the American Heart Association Diet plus standard of care. They’ll be on the diet intervention for a total of 16 weeks.
Bret:
Yeah, and this is really one of the first of its kind in this patient population, and I think it’s so interesting that you know to say, okay, we have the result in adults and will it translate to the same result in kids because they’re not the same?
Maybe the mechanisms of their psychiatric symptoms aren’t the same? Maybe the response to ketosis won’t exactly be the same? And also the feasibility may not be the same. what are some of the outcomes that they’re measuring to try and detect all these signals?
Kirk:
Yeah. The studies has three outcomes that they’re looking at.
One is looking at adherence and safety. We don’t know a lot about the use of ketogenic diet in young people with serious mental illness, or in this case, bipolar disorder. We know a lot about the ketogenic diet in young people with epilepsy, but this is a bit different. The condition itself affects how people relate to their families, how they relate to their social networks and just in society, in general.
Adding a big change, like fundamentally changing a diet is an unknown. These are young individuals, so they’re between ages of 12 and 19. So, their family is also a factor. Is the family going to eat keto or are they preparing just special meals for the kid? it has an effect and a dynamic both in the family as well as in school and in broader social life.
And we don’t really understand how that affects things like adherence. So that’s a really important part of it. Another outcome, of course, is looking at symptom improvement. Do these individuals symptoms improve over time being on the ketogenic diet as compared to being on the American Heart Association diet?
And then lastly, they’re looking at changes to metabolic health. So even apart from changes in bipolar symptomatology, do they see changes in things like BMI, insulin resistance, inflammatory markers, cognitive performance? So, we’ll be looking at these three outcomes across the study.
Bret:
Yeah, and that last point is so important because emerging evidence has clearly shown the increased risk of poor outcomes from metabolic consequences.
So people with bipolar disorder, actually dying from metabolic-related diseases more often than the general population. So addressing that risk early in youth seems like it could be a very important intervention. So, I’m glad they’re measuring that as well. And I like that it’s in foresight. If you don’t live in LA by UCLA, you can still take part in it.
So you said it was UCLA, Pittsburgh, Denver. And what was the fourth site?
Kirk:
Cincinnati.
Bret:
Yeah, very good. Yeah, I like how it’s very broad now, that is the traditional randomized control trial, that will be published and run out of research institutions. But there’s other type of data “research” that doesn’t quite fit that.
That category that you also have helped facilitate through the CMHRC, which is a very different kind of intervention and measuring of data. So, tell us a little bit about that as well and how that addresses the gaps in pediatric bipolar research.
Kirk:
Sure. So, the CMHRC is the Children’s Mental Health Resource Center.
It’s a national not-for-profit that provides service and support to families that have a member with a mental illness. It’s a really fabulous organization. It’s run by a woman named Elizabeth Errico, and her research partner in crime here, is a woman named Jana Cupp. And together they’ve asked themselves, they’ve noticed that these families that have a child with a serious mental illness really struggle and they’re always looking for ways to help improve their outcomes, their quality of life, better help support them.
They’ve seen some of the work being done around ketogenic diet and bipolar, and they really wanted to make this available to their constituents. So, this is really a pilot study. It’s a very small pilot study starting with five families, although they’ve already passed the five family marketer look to be recruiting closer to 10 families now, which speaks to the personalities and the ambition of the those involved and their desire to help people.
There’s a two week baseline period where they’re going to be measuring people’s metabolic health, health in general, just to make sure that things are stable and that they’re appropriate for ketogenic diet intervention. And then they’re going to train a family and the individuals around ketogenic therapy, and it’s a six month ketogenic diet segment that these individual individuals will be following.
I would say, although they’re collecting research data and there’s definitely going to be an evidence generating manuscript writing component of this, is really them just wanting to deliver a service for a community that has a need. And by embedding research in that process, we call it a learning health system.
They can learn the conditions under which it’s effective or it’s not effective. They’re doing some really interesting work. There’s the expected quantitative pieces, like blood ketones and insulin resistance and blood lipid biomarkers and so on. But it’s the qualitative piece that I think they’re going to learn the most from.
When you’re working with individuals between the ages of 9 and 17, there’s other dynamics at play, like I mentioned before. There’s the family dynamics, there’s school dynamics, there’s social network dynamics. How do those things factor into adherence to a ketogenic diet? Are there different ways of gamifying it so that kids can feel like they can engage in those structures effectively in social structures and family structures while still being adherent to their diet?
And I think they’re going to be learning a lot about what works, what doesn’t work, how families approach it to help support their loved one. So, I think there’s going to be a lot of really deep learning coming out of this really interesting study.
Bret:
Yeah, I think that is going to be really interesting and you can get some of that in a university-based academic institution, RCT, but not to the degree that you can with some of this more kind of “real world” data without sort of the confines of a research institution and six months.
Six months is a very long time in terms of a study of collecting data and following somebody for this type of intervention. So, I think it’s going to be very eye-opening. And how many parents are out there saying, could this be an intervention for my child? Is it safe? Is it effective? How do I do it? What are the tricks to get them to be more adherent and to have a better outcome? These are all questions that we have little signals on here and there, but to try and get it a little more, a stronger signal on is so important.
So, you said they’ve enrolled five so far and they’re continuing to enroll, and they’re nationwide, are they not?
Kirk:
They’re nationwide, that’s right.
Bret:
Yeah. So, we can definitely include a link to them as well. You’ve had a big hand in helping facilitate both of these studies, and that are going to generate really groundbreaking data on pediatric bipolar and ketogenic intervention.
So what do you see for the future in this field or maybe future studies or the ability to start offering it now as a treatment option?
Kirk:
This is a missing piece of the puzzle for us. Understanding how the ketogenic diet, whether it can be effective and issues around adherence in a younger population.
I think that’s absolutely critical and it’s just such a pleasure to get to work with Dr. Miklowitz and the team at CMHRC on the work that they’re doing. They bring such passion to the project. They really are doing this because they believe in their hearts that this is going to make a big difference for people.
And I think if we’re able to demonstrate, in fact, that this does demonstrate improvements in metabolic health, improvements in clinical symptomatology, that what that allows us to do is to speak to clinicians who work with youth and say, this should be a tool in your toolbox. Yes, there’s more research to be done.
Yes, we need to understand things even at a larger scale than what we’ve already done them. But it’s a promising tool that we have a hundred years of history on clinically that we think should be in the toolbox. As you’re working with individuals that have serious mental illness and as you’re discovering what’s working, what’s not working, this is another option that could be an incredibly powerful tool to use.
And I think doing studies like this really helps us craft that narrative and be able to say that to clinicians, that we’re not shooting in the dark here. We actually have some data we understand what the risks and what the potential benefits are.
Bret:
Great, thank you so much for going over those important studies with us and I look forward to hearing more from you in the future.
And, of course, we can always find more about you and our work at metabolicmind.org. So, thanks again.
Kirk:
Thanks for having me, Bret. Always a pleasure.
Bret:
I wanna take a brief moment to let our practitioners know about a couple of fantastic free CME courses developed in partnership with Baszucki Group by Dr. Georgia Ede and Dr. Chris Palmer. Both of these free CME sessions provide excellent insight on incorporating metabolic therapies for mental illness into your practice. They’re approved for a MA category one credits, CNE nursing credit hours, and continuing education credits for psychologists, and they’re completely free of charge on mycme.com. There’s a link in the description. I highly recommend you check them both out.
Thanks for listening to the Metabolic Mind Podcast. If you found this episode helpful, please leave a rating and comment as we’d love to hear from you. And please click the subscribe button so you won’t miss any of our future episodes.
And you can see full video episodes on our YouTube page at Metabolic Mind. Lastly, if you know someone who may benefit from this information, please share it as our goal is to spread this information to help as many people as possible. Thanks again for listening, and we’ll see you here next time at the Metabolic Mind Podcast.
Listen, Watch & Subscribe on:


Youth mental health refers to the emotional, psychological, and cognitive well-being of children, adolescents, and young adults. This period of life is marked by rapid brain development and…
Read more

The promise of ketogenic therapy for treating mental illness is accelerating with the newly published findings of a pilot study at The Ohio State University, which showed remarkable…
Learn more
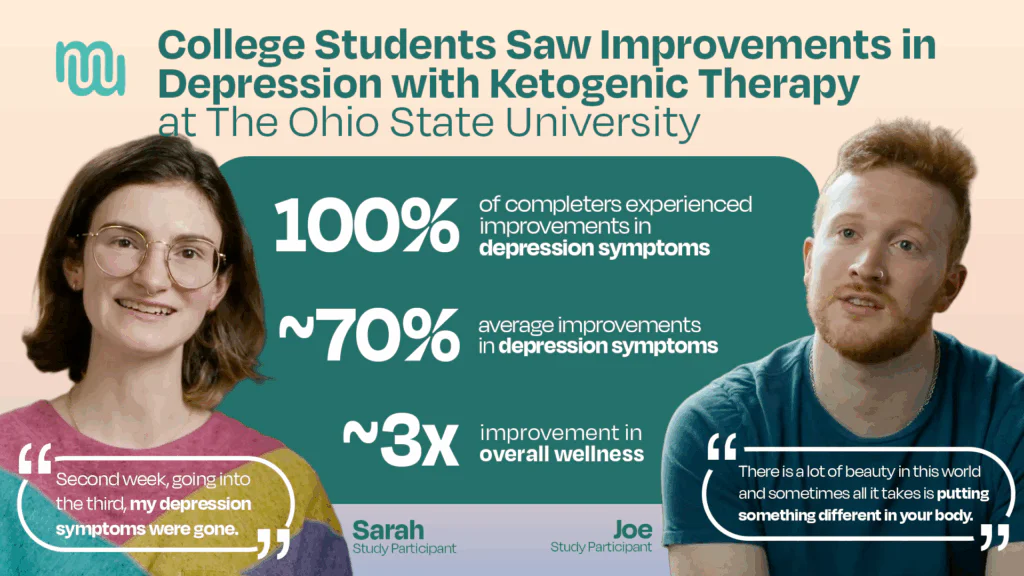
A new study shows an association between at least 10 weeks of following a well-formulated ketogenic diet and a roughly 70% decrease in depression symptoms among a small…
Learn more

Youth mental illness is on the rise, and treatment options are often limited, especially for kids with bipolar disorder. In this interview, Elizabeth Errico, founder of the Children's Mental Health Resource Center (CMHRC), shares how her organization is implementing ketogenic therapy in a real-world setting for kids aged 6 to 17. The year-long study is part of a larger initiative supported by the Baszucki Group to expand mental health care options through metabolic approaches.
Learn more
Youth mental health refers to the emotional, psychological, and cognitive well-being of children, adolescents, and young adults. This period of life is marked by rapid brain development and…
Read more
The promise of ketogenic therapy for treating mental illness is accelerating with the newly published findings of a pilot study at The Ohio State University, which showed remarkable…
Learn more
A new study shows an association between at least 10 weeks of following a well-formulated ketogenic diet and a roughly 70% decrease in depression symptoms among a small…
Learn more
Youth mental illness is on the rise, and treatment options are often limited, especially for kids with bipolar disorder. In this interview, Elizabeth Errico, founder of the Children's Mental Health Resource Center (CMHRC), shares how her organization is implementing ketogenic therapy in a real-world setting for kids aged 6 to 17. The year-long study is part of a larger initiative supported by the Baszucki Group to expand mental health care options through metabolic approaches.
Learn more