Share your story. Help someone else start theirs. Share Now

Listen, Watch & Subscribe on:



The Hidden Drivers of Anxiety and Depression in College Students
Listen
About the host

About the guest


Bret:
Dr. Ryan Patel, a senior staff psychiatrist at the Ohio State University, has dedicated his career to focusing on mental health in college-age students in such a unique population. They’re not pediatric patients, but they’re not really quite yet adult patients. They’re in that middle ground where so much is changing, and Dr. Patel talks about these changes and the lifestyle changes that can impact those who perform well in college or those who end up dropping out. He talks about his five most important interventions to address in this population to help them achieve success in their mental health and in their college career.
And we also talk about his involvement in the kind trial, the ketogenic intervention for college-aged students with depression, and now maybe the results of that have impacted his approach. This is a tour to force on how to approach college-age mental health. So I hope you enjoy this interview with Dr. Ryan Patel. Dr. Patel, thank you so much for joining me today at Metabolic Mind.
Ryan:
Thanks for having me.
Bret:
I’m excited to talk to you about college mental health, specifically mental health in people who are attending college and of that age, because you’re an expert in this field. But before we get into that, give us a little bit of your background, um, how you came to be an expert in college mental health and where you are and what you’re doing.
Ryan:
I’m a college psychiatrist here at Ohio State University and the Office of Student Life Counseling and Consultation Service. I’ve been here about 10 years. In addition to that role, I also oversee our research operations and I’m chair of our department’s research committee. And so our projects have typically focused on college mental health and, in particular, clinically oriented research projects.
And so, you know, I really got enamored by kind of the developing young adult and helping them. Become their best and enter the professional realm, and you know, become productive members of society. And you know, one of the things I realized over time is, you know, for a lot of individuals, you know, a lot of people have a heart attack in their forties and fifties, right?
And maybe sometimes older. And by that point, you know, you have been kind of living in a certain way and have these health behaviors that are kind of set. What I started to recognize is, you know, that’s a lot more difficult to change than, you know, let’s take a college student or a young adult, who is out of the house and trying to figure out life and, you know, get them on a solid foundation right out of the job.
And so, you know, that kind of, uh, further fueled my desire to work with college students. Let’s get young adults on a trajectory of total health. Right from the foundation. And my belief is that would help change the total trajectory, the healthcare cost curve of that individual across the lifespan.
And the more we do that with young adults, you’re really talking about shifting the issue of health problem that we have in our country. And in the vast majority of it is. Through, uh, as a result of chronic disease, right? And chronic disease, how you live and lifestyle factors play a big role in that.
And, that’s really how and why, you know, I kind of became more and more enamored with working with young adults and college students, and, you know, not only are they developing these health behaviors. They’re also kind of developing an outlook of the world and how that works and, you know, what you learned in school, what you learned at home, and how do you reconcile that with the realities, how, how the world operates.
And so, you know, now you’re also addressing the operating system that could help that young person long term. I also started a blog and I intentionally don’t write about medications, you know, and what I saw when I looked at the analytics and things is, you know. Students look at it for about 30 seconds or so, right?
So, right. You gotta get to the point, right? So I, I try to like, pull out a study, how can you apply it to everyday life? And the idea was just over and over. I’m hammering the point that there are things you can do in your everyday life to improve your mental health. And, you know, I, I do believe that what we need to do is.
Have an impact on a larger scale. There’s not a lot of psychiatrists, there’s not a lot of providers who have this kind of a mindset and this kind of an approach, and a lot of people are suffering. And so, whether it’s the blog or the book or my involvement, you know, I’m the chair of the mental health section of American College Health Association.
It’s really that how can we do things at scale to benefit, mental health of our young adults.
Bret:
Oh, so that there’s so much in there and I think that’s really interesting, your path and in such a unique population, right? You think of there’s maybe pediatric psychiatrist and adult psychiatrist, but here’s, there’s.
There’s this middle group. I mean, I guess they’re considered adults ’cause they’re over 18, but they’re really not quite into the world. Adults. And as you said, so much about their mindset and their approach to the world is being shaped in this time. And, you know, so many things have changing. Maybe they’re living outta the house for the first time.
They have the stresses of school, they have the stresses of being more independent and, and not having maybe as much control over their lifestyle. There can be an introduction of drugs and alcohol and substance and sleep deprivation. So all these things change. So I mean, what do you see as some of the most pressing challenges that face the college age individual that you don’t see in general pediatric or general adult psychiatry.
Ryan:
Yeah, so there’s a number of them, you know, and so. One, one of the things to, to highlight there, which is that there are some unique things happening at that 18 to 24 age range, and so much so that I think the FDA is kind of moving towards having a separate category, looking at young adults, you know, so we look at drug trials and things like that.
They’re even saying, you know what, this is, uh, a, a different population and thinking about. Young adults in particular, categorically, whether they’re college students or not. You know, one of the things that we’re seeing is the way they’re living their lives is just not healthy. And we can kind of, drill into some of the data to support that uh, as the opportunity allows.
But that’s one issue. Okay. But the second issue is, you know, thinking about this college student. What has happened is, you know, if you look at, for example, test scores, GPAs, you know, they’re very smart, and if anything, those numbers continue to improve, yet you see this decline in mental health.
What, what, what’s going on? One of the things, uh, you think about is, okay you know, you think about. Students spending more, you know, at least the college students coming in, you know, maybe you’re spending more time in school in high school and things like that. Study. Okay, great. They’re also using, you know, technology for entertainment, all these other things, but who is making sure they go to bed on time?
Who’s doing their launch? Who’s doing the cooking? Who’s doing the cleaning? Who’s buying the groceries? All this stuff. Um, all these life behaviors, somebody else is figuring out. For there. And now they’re in this environment where they have to figure all that out for themselves, and there’s a skillset set that’s missing.
Okay. So that’s one aspect of things. Second aspect of things is, you know, you have these young adults who are learning. I’m not sure if that’s the right word, but, you know, when you think about like technology and social media and things like that, you know, it’s, you gotta be the perfect and the best in, best in the world at something, or your failure, you know, so there’s this kind of all or nothing mindset, you know, that, that people come in with.
And then you extend that further into this idea that, oh, I gotta go. All in, you kind of going all in and you know, school is the only thing that’s boring. Oh, what about sleep? What are you eating? All these other things, you know, activity factor, all these things. Just kind of fall as secondary when in reality, when you live in a healthy way, your brain functions at its best.
You do your best and you can actually become your best. You know? So, there’s a, a disconnect of, not prioritizing health behaviors because they didn’t learn that, you know, they don’t learn that in school. They’re not learning that, uh, categorically at home and, uh, you have this issue of life skills that’s also missing.
And so that, you know, that you put that individual now in the college environment, you’ve got a problem.
Bret:
Yeah. And so what, how do you see that manifest? I mean, is it, is that part of what’s, um, contributing to the rise of anxiety disorders and depression and maybe even OCD or a DD? Like, do you see those lifestyle deficits as major contributors to what you see in terms of the psychiatric manifestations.
Ryan:
Yeah. So when you look at, for example the American College Health Association does this national college health assessment. This is a, a representative sample of college students from hundreds of universities across the country. And this is rolling data, twice a year that we pull this data of students.
Right. And when we look at that, for example, one of the things you see is 80% of students are sleeping less than seven hours per minute. Okay. Recommended amount of sleep for young adults is between eight to nine hours. You know, it used to be eight and a half to nine and a half hours, and it kind of rolled that back a little, but eight to nine.
Okay. Vast majority of college students are reporting. They feel tired every day, okay? Uh, they’re not getting enough sleep. And we know for example, that the risk of academic failure is defined by GPA less than 2.0 significantly increases when you don’t get enough sleep. Okay? Second part of that is, you know, you look at depression, anxiety, substance use, all of those things significantly increase what an individual is not getting enough sleep.
Add to that, uh, suicidal ideation. There was a study done in college students looking at individuals that are not depressed, okay. They’re just not getting enough sleep. Okay. And what we see is a 2.5 times greater odds ratio of having suicidal ideation in suicidal behaviors in young adults when you’re not getting enough sleep.
You know, that’s just one element of it. Okay? The, the second part is, you know, several systematic reviews have shown, uh, one of them review of over 20 different studies with over a hundred thousand sample size showing that, sanitary behavior increases anxiety. Similarly about 30 different studies looking at uh, physical activity and depression show that there is a bidirectional relationship between sedentary behavior and depression.
So we see that, you know, okay, you’re, you’re, you’re not as physically active. You’re not getting enough sleep. You know, there’s this, this sort of a stereotype of, you know, there’s a coffee shop at every block and there’s a vending machine in every building, and what are the hat, caffeine, energy, drinks, you know, all these kinds of things.
So now you’re taking a highly sedentary individual that’s not physically active, that’s not, you know, we’re talking about nutrition shortly. And, you know, they’re, they’re just caffeinated. Well, what’s that gonna do to your anxiety level? What’s that gonna do to your sleep? Um, so you have that factor going on.
Uh, you have this issue of, uh, technology use, so when you think about like pre pandemic to now you know, one of the things that, what were the big three that young people were doing right? Netflix, YouTube, and maybe a video game or social media, like that was like the big three, right?
If you’re on your screen all day, you’re doing technology work all day, and now you’re trying to use those things to have sort of a mental break you know that’s not really gonna work. You know, you’re kind of using the same brain muscles and eyes and all of these things to just sit more when you’ve been sitting a lot all day, so you have this kind of a issue of, okay, what do I do instead? And people, you know, think of these as toys. These aren’t toys, these aren’t benign things. You know, they can be. A powerful tool or a dangerous weapon depending on how it’s being used, you know, and in the context in which is being used.
So you have that issue. Uh, looking at nutrition as an example. So there’s, uh, 21 different studies from 10 different countries talking about nutrition and how it can uh, reduce the risk of developing depression. Not only that, but there’s a similar size systematic review looking at. Nutrition and its effect on anxiety.
And you know, if you just go to the minimum of, fruit, vegetable protein intake, things like that just the basic guidelines you can improve anxiety symptoms. Okay. There’s at least been five different trials looking at nutrition just to treat depression. Uh, and number of them shown at least a 50% improvement.
Ours has shown a little bit bigger, but it’s a pilot study. We’ll, we’ll discuss that later, but food intake. Okay, so let me go. Go to that. Okay. In our college students, on average, 70% of college students get about two or servings or less of food per day. 80% of college students are reporting food insecurity.
Um, when you look at the health index, just based on the dietary guidelines for Americans, college students are at 56 out of a hundred. That’s not a passing grade.
Bret:
Yeah. I mean, that’s a lot. It seems like that’s a lot to consider, uh, so many different influences that in a way have just become normalized.
Like everything that you’ve mentioned is sort of like Yeah. It’s just, uh, that’s the way life has gone. That’s the way it is. And you know, I can see how people just sort of normalize, Hey, I’m getting seven hours of sleep. I’m not eating well. You know, I’m kind of stressed out and not moving much, but that’s, that’s life.
You know? That’s the way it is. And I think that’s, it’s frustrating to see how many people can normalize that.
Ryan:
And you know, when you look at treatment availability and things like that. Okay. So there are students that have, you know, when you think about like severe mental illness and things like that, base rate of that has not really changed a lot.
But the suffering of college students has gone up a lot, as evidenced by depression rates, anxiety, stress and things like that. What I posit is, the big reason for that is all of these lifestyle factors, which will help individuals with chronic mental illness as well as all the other students that are reporting mental health problems.
So you have those two factors and what are schools doing, you know, so, uh, what our lot of schools are doing is focusing on, okay, we need to address the treatment side of things. Okay? Students do need that, but you know, that’s not this 80% right. So we, we also need to address those things. But the wellness programs and things like that, different schools have them in different capacities, but they’re not these systematic focus on these key outcomes and let’s align all of our resources to do this at scale.
You know, and that’s kind of the missing gap.
Bret:
And like you’re saying, if the focus then is on medication treatment rather than lifestyle prevention. There’s a big disconnect there, but at the same time, so everything you’ve talked about is, is so pertinent for college aged students, but it’s also the age where we see sort of the spike in bipolar disorder and schizophrenia diagnoses.
Now you said it, that hasn’t changed much, but it still. In that age group. So how do you think those lifestyle factors play into that being the age group where we see the onset of serious mental illness?
Ryan:
Yeah, so, you know, important point there, which is that we see a lot of uh, serious mental illness evolving and occurring at this age.
And so that is, that is a very important reason why we wanna make sure, and I big advocate for making sure that. Treatment resources are, are available on campus. And a big reason is, you know, things evolve. Right? You know, what might start out as, you know, panic attacks ends up as schizophrenia and, you know, how do you help a young person, reconcile all of that and stay in treatment so that we reduce the duration of untreated psychosis.
We do the early intervention so that their condition doesn’t end up worse. You know? ’cause there, there, that’s the thing in schizophrenia, as you know, the, the sooner you recognize, the sooner you treat it. The more likelihood that you can modify the long-term trajectory of that condition. When you think about bipolar, a similar issue, right?
So when you think about, as an example, individuals with bipolar disorder, you know, there’s such a thing, you know, like when you disrupt circadian rhythms, you increase the likelihood of having a manic episode. Every time you have a manic episode, that makes it more difficult to treat over the long term.
It’s, you know, thinking of it, a toxic event to the brain and so on. And so, yeah, if you’re sleep deprived, you’re over caffeinated and you’re not eating properly, you know, those things are going to contribute to, uh, that condition not being as well managed. And then the second part of that is, you know, we think about.
A number of medications that we use for chronic and severe mental illness. A lot of times these are atypical antipsychotics and those types of medications that do have a side effect profile. And a big one is metabolic side effects, right? And, you know, what do you what is the number one killer of individual schizophrenia?
Consequences of metabolic syndrome. You know, it’s a heart attack. It’s, those kinds of things are in their fifties and things like that. And so those lifestyle factors also. Play a role in those situations.
Bret:
Yeah. Yeah. That, that makes a lot of sense. Well, I mean, you certainly outlined the problem and it, it seems almost, too much to tackle and for, for college age kids without a lot of control, with maybe, without a lot of insight where a lot of this is normalized.
But then in your blog and in your book, you outline a number of different, hacks and, and interventions and lifestyle changes that are research based. I thought that was so interesting about your book that you mentioned there were a over a thousand studies looking specifically at college-aged individuals.
So, so what are some of the highlights of the specific lifestyle interventions that someone can institute today that are evidence-based to reduce the onset of psychiatric symptoms and illness in the future?
Ryan:
Well, one of the first things is. As I tell my students, you know, I do a program, I’m on, on, on these key five key things that I’ll discuss.
The first one is you have to get enough sleep. You know, there’s really nothing that you can do to counteract. Problems of sleep, de sleep deficit. You know, you can drink more caffeine. It’s gonna keep you awake. Your brain’s not gonna work as sharply as I pointed out in some of my blog posts related to, energy drinks and so on, right?
And so one of the things to recognize is, you as a young adult, your brain and body is still developing and you need. Enough sleep and at least, you know, the recommendation is seven to eight hours. Uh, sorry, I’m sorry, eight to nine hours. You know, you really need to, it’s not a good idea to fall below that.
One, get enough sleep. Two is nutrition. There are many nutritional things, but you know what the research shows is focusing on key foods. That have nutritional density, right? So thinking about eating your fruits and vegetables, getting enough protein, you know, trying to avoid, um, excessive caffeine intake, trying to you know, avoid ultra processed foods doesn’t mean you can’t have those things but rather that those are more of an accessory than a core, thinking about that, you know, like, and as I say, you know, like sometimes I don’t wanna eat my vegetables, but you know.
When I do, I feel better. You know? I know that I’m going to feel my best and I’m going to. A function at my best if I give my body the nutrients that it needs, and to kind of reframing that into, okay, can I at least get a protein or fruit or vegetable as part of my meal? If I do that for three meals a day, I get to my minimum of five servings of fruits and vegetables a day.
Now, which of those fruits, ve that’s, you can choose that, right? You know, if you don’t like spinach, maybe you, you don’t eat that. Right? Eating a vegetable is still better than, not eating those kinds of foods at all. So getting those, you know, thinking about nutrients, uh, and, and thinking about that and, you know, different people do best on different dietary clans and different meal frequencies and things like that.
Sure. You know, and you can kind of think about what works best for you, but can you at least try to prioritize these nutrient dense foods, number one. So we’ve got sleep. We’ve got nutrition, and the third part is physical activity. And I, and I just say, Hey, you know what, uh, that, that systematic review that I was talking about, one of them was talking about sedentary behavior and anxiety, and one of the measures was less than 6,000 steps a day.
You all have a phone. You all have a phone, okay? There’s a free app you can get. I have it on my phone. You know what it’s called? It’s called pome. It’s a free app, okay? And it shows me that now if you’re feeling anxious and stressed and your step count is below 6,200, okay? You know what? Maybe as a coping mechanism, I need to make sure and get that minimum activity.
Uh, you don’t have to necessarily engage in a structured exercise regimen if that is not something you wish to do, or time doesn’t allow that. But can you at least try to get, you know, your step count at least to a minimum? So those are, that, that’s another part is physical activity.
There are certainly added benefits to engaging in a well-formulated structured exercise regimen or playing in team sports and things like that. There are social benefits and things like that you gain, so certainly those are added bonuses, if that’s something you can do, but at least not, get that physical activity to a minimum, right? That’s, I’m not talking about going too much minimum. So we’ve got sleep, nutrition, exercise and then the other part is healthy ways of engaging with technology. So as I discussed, a lot of students are spending more time than is beneficial for their mental health.
When I think about discretionary technology use, so what I recommend to students is, you know, thinking about first is, you know, instead of saying what’s, whether technology is good or bad. Thinking, maybe reframe that into, it’s how we use technology. So how did you feel after doing certain things like that?
Is it helping you feel better going to a particular app or playing a particular thing or so on? You know, kind of become mindful of your use, reflect on that and if, if you go to a particular site or do a particular thing with technology and you end up feeling worse every time. Maybe you scale back on that, and it doesn’t have to be permanent.
You know, maybe, maybe it’s not good for you today. Maybe less is good for you today and more might be better for you tomorrow. But start thinking about how it’s making you feel and calibrate your intake. And then the other part I discuss with students is, you know, thinking about setting a limit on that.
Why? Because your ability to read and process, do cognitive work is limited. You know, you get this much, I’m pointing to a, a canister here. You get this much cognitive power a day. Do you wanna use this much of it on entertainment and this much on classwork, or do you wanna finish your classwork and use what’s left for entertainment?
You choose, we don’t have infinite brain power every day. Our brain can only do so much of cognitive work, right? So can you set a limit? And the limit that I recommend to students is setting an hour, no more than an hour of discretionary screen time per day. Now, some professional guidelines and things like that are, are talking about more like two hours.
Uh, so why do I say an hour? A, because it’s gonna force you to prioritize what is it that you actually enjoy from these technology uses, right? What is it that you wanna keep? Okay. And b, setting that time limit will force you to take care of yourself and enjoy life in other ways. As I’ve discussed all of these, all the ways that young people are, uh, not so good about taking care of themselves, you know, food, sleep, exercise, other ways, you know, these are activities, you know.
Spending time with friends, you know, those kinds of things. So what it will encourage you to think about other ways, you know, cooking, you know, drawing, painting, you know, there are other ways that you can kind of soothe your brain and de-stress, and there’s a lot of research supporting that. So this setting, that time limit will actually free you to pursue those things.
Uh, and lastly, uh, you know, the more time you spend on technology for entertainment, it also has the effect of. Displacing the time from sleep, and again, if you kind of add that limit of technology and focus on what’s actually meaningful to you, you’re gonna sleep better and get that sleep that you need.
And so, those would be the big ones.
Bret:
Yeah. I mean, I can see how each one of those can be so impactful and at the same time, they’re incredibly common sense. But seemingly incredibly difficult to change in someone of that age group who’s been doing this for so long and has been normalized for so long.
And so, I mean, what’s the reaction when you talk to somebody about this? I don’t know. I’m just trying to think of me talking to my kids about it. It’s like, yeah, yeah, yeah, I know, I know. And they just sort of blow it off and really don’t think it’s, it’s all that important. Like how do you really get them to sort of just sort of internalize and, and see, oh yeah, this is going to really make a difference, or this can make a difference and this is important.
Ryan:
Yeah. So a couple of things, you know, first is, what I just said is not something that they’re learning anywhere else, right? They’re not learning that in school, in middle school or high school, you know, on average. On average. They’re not learning that at home on average, again. They’re exceptions obviously, but, and similarly, they’re not learning that at most places in Canada.
You know, there’s also, most people don’t know, you know, we have not as a system, as a. As a nation, as a school, as a community, made these things a priority. You know, and they’ve just fallen off over time, right? Nobody intentionally meant to do this, but here we are, you know? Um, and so what, what helps is, when I talk to students about it, you know, I’m, I’m seeing a patient or something, you know, I’m discussing the why, why do you need to eat in this way? You know, your brain needs to make serotonin and dopamine, these neurotransmitters, well, you can’t make those without vitamins and minerals. You can’t make those without protein, so that’s why you need to eat those things. If you don’t eat those things, and I’m gonna give you medications, they’re not gonna work as well.
You’re gonna have side effects. A lot of times students don’t wanna be on medications, right? If you wanna see a future where you’re not having to take these medications. Here are things that you can do so that you do feel better. So my point is what helps is explaining the why. You are having anxiety problems and in your case, your caffeine intake is too high.
Your case, you know, you’re not sleeping enough. Uh, and you don’t have to take my word for it. Try these things. If it doesn’t work, you know, then we know that it’s something else. And so, you know, kind of putting the onus back on the student that hey, you know, connecting the solution to the problem, right?
You’re here for a particular problem. The path to the solution is these things and these things will happen. And discussing the effect size, you know, 50% improvement. You wanna be 50% better without having to take a medication. That sounds pretty good to me. Uh, a third of people, you know, go into remission ’cause they ate better for depression.
Okay. That sounds good to me. But also explaining these neurotransmitters and things like that, that’s something that students understand. And, you know, our our students that as I mentioned previously are, are very smart. Right. And they’re very much they don’t wanna know opinions, you know, they want to know the data and things like that.
So I can show them the research and I can discuss that and that I think is also very helpful. In driving that behavior change, and that it’s not all or nothing, but can you just, can you decrease a little bit and see for yourself, that,
Bret:
And when you’re talking about the data, is there data correlating the, the risk of dropout with.
The symptoms of anxiety and depression, or even with the sleep deprivation or, or technology use or, or whatever lifestyle you pick, is there that data correlating with the risk of dropout from college, which obviously will then significantly change someone’s life trajectory from there?
Ryan:
Yeah. Excellent question.
So yes, so, uh, going back to a CHA data you know, they’ve looked at what is the reason why a college student drops out and there are two sided. Number one reason why college students drops out is actually finances. And, you know, they feel the financial pressure. Uh, and the second reason is mental health problems.
And the difference is about 54 to 40, 40 something, you know, so it’s pretty close in terms of why. Um, and, uh, the other extension is, you know, when you ask young, uh, when you ask college students in these surveys, what is. What is the impediment to your academic performance? The number one impediment that caused students cite to their academic performance is mental health.
So to connect these life behaviors, we know these life behaviors improve these mental health symptoms. And if you’re saying your mental health symptoms are what is affecting your academic performance and you are doing well in school. There is the connection looking at characteristics of successful students.
Okay, so that, that this is, uh, this was a study done that came out a few months ago. I think it was looking at, high performing college students and what are their life behaviors and it’s, you know, and it looked, broke it down by GPA and, you know, looked at sleep, nutrition, exercise, screen time, and it’s all the things I’m talking about.
You know, that those high performing students are getting enough sleep. They are exercising, they are eating their two servings of fruits and, uh, five servings of fruits, vegetables today, so on and so forth. I mean, it’s, it’s pretty striking.
Bret:
Uh, so now I wanna narrow in a little bit more on nutrition. I mean, I think we could spend an hour podcast on any one of these things, sleep, technology, movement, et cetera.
But I, I wanna talk a little bit more about nutrition and I think it’s clear that we can all improve. Our mental health by improving the way we eat, cutting out the ultra processed foods, the high sugar foods, the refined carbohydrate foods, and like you said, eating more protein, uh, getting your fruits and vegetables.
But now you’re at Ohio State, so you are in a, a, a unique institution that has some of the foremost. Ketosis researchers on the planet. So, you know, there’s Dr. Jeff Ick working with his nutritionist, Taryn Bedell. And, and now you’ve got Dr. Madison Kackley and, and Drew Decker as a research associate. All these amazing minds working on ketogenic nutrition research and.
Having worked on the KIND trial, specifically looking at a ketogenic intervention in college age students with depression, which had some pretty impressive results in terms of the impact seen by improving depression symptoms with ketosis. So when you see something specific like that, yes, eating better can help, but then going the next step towards putting somebody into ketosis through a dietary intervention.
And seeing the results that can have, even though it’s a pilot trial, how has that helped shape your approach to say, well, maybe we need to be a little bit more specific about nutritional advice in some subsets of college age students. How’s that changed for you?
Ryan:
I’m so glad to have participated in, in this study.
You know, I saw the students be, you know, pre pretrial and, and then during this, during the study I see them and things like that. And. You know, when we look at the evidence basis for, you know, nutrition for depression specifically, the most amount of research, uh, supports what’s called this Whole Foods Mediterranean style Diet, uh, eating okay.
Eating pattern. Generally speaking. And while that is the case, not everybody as I’m, as I mentioned previously, right? Not everybody. Does well on the same kind of eating pattern. You know, some people function better and they feel better, you know, on a higher carbohydrate eating pattern.
Some people do better actually on a higher protein. Some people do better on more of a ketogenic type eating pattern and things like that. And so there’s a, there’s a variation in the population on who does best eating what kinds of foods. The second part of that is that. With our, our study in particular, and, and what the role there is, you know, is young people are actually, conscious and, and, and, and interested in learning about ways to improve their nutrition.
Let OSUI do a nutrition program, food strategies for depression sleep, uh, food strategies for focus, food strategies for anxiety. Sleep and exercise strategies for mental health. And over the years, you know, it ends up being about a thousand students a year that opt into it, to learn about this kind of thing, uh, which is really great, right?
But it also I think, kind of highlights the interest of students in think, you know, being more thoughtful about what it is that they’re eating. Okay. Second part of that is that. There is quite a bit of research with, well formulated ketogenic diets for a variety of health conditions and in particular kind of inflammatory disease and chronic disease and things like that.
And as I discussed, you know, with our population, you know, we do have this issue of we’re on living in the most healthiest way, with regards to a variety of things. And so, and, and we see students over the years that are already, uh, doing keto and things like that. And, and what’s been missing is, hey, you know, we don’t really have any guidance on what to do.
If I encounter a, you know, if I see a student for the first time and let’s say they have depression or something in they’re keto should I get them off that? Or is it okay for them to stay on it? We don’t really know. And the other issue that, you know, I, I see frequently is, you know, uh, individuals that do try going the ketogenic way is, you know, it’s not well formulated.
They’re not paying attention to their electrolytes and they’re not doing the things that you’re supposed to be doing. You know, when you kind of go. Keto, it’s you have to do it in a way that that works, right? There’s some moving pieces to that, right? That’s why it’s a well formulated keto.
And so, explaining that to students and so it’s been, I have felt that, you know, one of the benefits of even before our study is there’s something here because of the way it affects inflammation and the way, you know, it’s been shown to be beneficial in so many conditions and. Um, how does it stack up to this Whole Foods Mediterranean style, which again, not everybody likes, so not everybody wants to be on, right?
So, and so. Anyway, so that’s kind of where we were with the study, and it was really exciting to see how powerful the results were.
Bret:
Yeah. And not just how powerful the results were, but just the ability of college age students to get into ketosis and stay in ketosis for the duration of the study.
I mean, I would’ve thought that this would be a, a very difficult age group. Where the dropout would be really high, and that wasn’t the case. Now again, a pilot trial that wasn’t randomized, so, you know, with those caveats, but I think that’s really encouraging. One, to set the stage for future research, but also to say, okay, there’s really something here that if, if I work with this college student to help them understand what a well formulated ketogenic diet is and give them the support that they need, that this could have a dramatic impact on their mental health And, and like you said.
Up to this point, the research has basically been in, in a Mediterranean diet, which can be, you know, defined in a number of different ways. You can have a Mediterranean keto diet and so forth. But I guess the question is if someone comes to you and they are suffering from depression symptoms and they’re not really paying attention to how they eat.
Do you think ketosis is one of those interventions that should be discussed within the first couple meetings of this individual? Or do you think it should only be reserved for maybe the refractory cases or, you know, people who have really struggled with other interventions? Like where, I don’t know if you can even answer this at this point, but where is it on your list of interventions that you wanna discuss with somebody?
Ryan:
Yeah, so, when I see somebody for the first time and they have depression, you know, we’re looking at everything. You know, we’re looking at. Not just their symptoms, but all, you know, making sure they don’t have other comorbid things asking about their medical history, addressing that, you know, their developmental history and, and so on and so forth.
But also looking at their lifestyle behaviors. And so what my ultimate goal of that evaluation is, what are the static and modifiable factors that can help improve the person’s depression? And that could be a variety of things. Or medications, you know, and I explained that to the student that, hey, you know, in your case there’s a role for medications and there’s a role for these things.
Or in your case, you know, if you do all these other things, you might not need to take medication. You know? Uh, and then it’s up to the student say, okay, I, I will do that. Now, out of all those things in your particular case, you know, thinking about what is the effect size of what you can do to improve your mental health, but the research shows that the biggest one is nutrition. What we didn’t know is, you know, a lot of times, you know, we do see students that are already trying to improve their health or are already trying to improve their nutrition. They, you know, they maybe have tried keto or they’re are on, you know, on keto now, that kind of thing.
Uh, then the question for me becomes, well, okay, is it well formulated? You know, what, what kind of macro, what are you eating exactly. You know, is it. Junk keto or is it, you know, a nutritious foods keto. Right. What about your electrolytes? You know, are you keeping it, paying attention to that and those kinds of things.
Right. With the benefit of the study and, and I think what’s been so helpful is at least we can say even though this was a pilot study, that you know what, at least we can say nobody in our study got worse. You know, nobody needed more medications. Nobody need to be hospitalized. And so at least, from what we know from this single study that we’ve done is at least we have that, to guide the student and not necessarily discourage them, but encourage them to make sure that it’s well formulated, that they’re, based on appropriate nutrients and not, you know, as I said, just.
Quote unquote, jock Keto.
Bret:
Well, and not only did they not get worse, but it seems like you just about everybody had significant and clinically significant improvements and you know, as being the one, taking care of them and seeing them as a clinician. I mean, were you, were you surprised by the results that you were seeing and the improvements you were seeing in, in your patients?
Ryan:
There were two things I was not expecting to see. The first one is, okay, so all, there’s all this research on the sort of the Mediterranean style that and things like that. I mean, and, and we look at the trials that were done, you know, by JAK and colleagues, you know, they were intensive, that involved a lot of education, a lot of intervention, providing food and all these kinds of things for a long time.
And and they saw, pretty good effect size. It was 50% improvement and a third went into remission pretty good randomized trial. And so, you know, part of it was okay, you know, I, I didn’t quite know how this would stack up. And what was, IM impressive to me, uh, from the study was that actually the results were.
Way better, than what I had expected you. It was a beyond 50%. I think I, I’ll have to go back and look, but it was something like six 70%, maybe higher. Uh, and so, uh, that was really remarkable that okay, you know, this does need to be looked at further and, you know, uh, this is a even better, because the effect size was so significant.
The second part of that is, you know, what I had thought about is, you know. Maybe we would see more of a effect size or the students that would benefit are the ones that perhaps already have metabolic syndrome or high levels of systemic inflammation from chronic disease, that kind of thing. But what was impressive from our study was actually no, we even had students that were kind of already healthy-ish, you know, kind of already mostly pretty fit, uh, already, you know, on decent, you know, nutritionally not doing excessive caffeine or drug use or alcohol or anything.
Even they saw improvement in a significant manner. You know, so it was not just kind of that metabolic syndrome type patient that saw improvement in their symptoms. That was striking. That was really striking to me. And then the other part that was really striking is, you know, uh, there were some patients that, um, uh, again, we’re kind of physically healthy and kind of do, decent with their lifestyle in terms of exercise and nutrition.
And, you know, their basis for depression was more more of a psychological basis, if you will. Okay. So have been depressed for a long time, you know, kind of chronic and existential, you know, these kinds of things. The kinds, the kind of depression that you would think, oh, you know, like this is a psychotherapy type depression.
And what was striking to me and really unexpected finding was. Their symptoms got better and I was, I was really surprised. And not only did they got better, but they got a lot better. And here you have a psychological basis for their, ideology of depressive symptoms and yet their depression got better on keto.
You know, like, what, what’s that about? Like that was really different. Uh, and you know, tho in those cases, it wasn’t like the students were on. More medications or something like that, the change was this and while they’re still, you know, engaging in their other recruitment. Okay.
Bret:
Well, yeah, and it’s interesting that you, you know, bringing up the Smiles trial the 12 week intervention of a Mediterranean diet versus basically no change in diet, but social support. So, you know, again, it’s improving the way they ate. So not a surprise that they got better. So did it, was it the Mediterranean diet or was it just improving the way they ate?
So now that sort of sets up this, well, how about a keto versus Mediterranean, or even a keto Mediterranean versus a non keto Mediterranean. Like that’s sort of like the, the natural next step. So, um, I know you at Ohio State are very busy with future studies, so I wonder if that would be one of them, or, you know, maybe you could answer that or tell us what else you’re working on that we can expect from you next.
Ryan:
Absolutely. So that is definitely something that would be, I think a very useful contribution that we could make to the field and, and really to society is, you know, how do the two compare? Uh, and not only how, how do the two compare, but is the effect size different? Because that’s something, right, you know, you, what you are doing with, with growing, ketogenic is.
Biologically different than, you know, a Whole Foods Mediterranean, non keto, right? And so what, what does that look like? And is there some signal differences outside of, you know, you’re just eating better quality food? And that question I think would be really, really powerful. Other things, you know, so what am I up to?
You know, one of the things that I’ve been trying to do is trying to take this message up. You know, we have these evidence-based lifestyle behaviors that improve mental health or college students. How can we. Engaged the entire college ecosystem into that. So that means the housing, housing settings dining halls, you know, student wellness programs, right?
Peer education. So I’m trying to partner with other organizations to disseminate that. And then the second part is how can we, as their professional organization prioritize these key health behaviors and say, okay, this is what we need to do. Now, the research that needs to go into is. What are the system level things that can help the individual make a better food choices?
B, so that they get enough sleep, maybe there’s quiet hours, maybe that exam deadline is not at midnight and then turn around and go to eight o’clock classes. Right. You know, so these kind of system level things and c you know, can we kind of come up with sort of general principles that all schools can follow?
Adding and adjusting based on their unique campus needs and their unique student population. You know, when I was at the Cleveland Clinic, they started implementing things at that time, at a system level, at the Cleveland Clinic. And that, I saw it for myself that, hey, you know, uh, when I’m on call and I gotta go grab a quick bite to eat from the cafeteria and go see the next patient.
Oh, I have some food choices now. That actually looks pretty good. You know what? I’m not gonna go do this day. I’ll, I’ll take this. And I saw for myself that would modify. My behavior because of the choices that were provided to me. And so, you know, you think about that on, on campuses, right? We could do that for our students as they’re developing these habits long term, so, uh, that’s kind of what I’m working on.
The last thing I’ll mention is technology use. Uh, I mentioned that it’s not that technology is good or bad, it’s how you use it. I think in the wor in the age of ai, there’s a next step, which is how can we help ai. So that it is supportive of mental health and positive coping.
And so that’s something that I’m working on, is I’m working with developers of AI based mental health support program, uh, that is available to students. And what I see from that is, you know, uh, not just providing the student in the moment support if they can’t find anybody else, you know, it’s night, you know, you’re in your room by yourself or something like that.
But also, you know, helping them with, uh, positive life behavior specific to that person. You know, so like going back to that example, you know, they’re on that AI at midnight and hey, you know, the AI recognizes that, Hey, man, like you have not been sleeping. You know, you actually need to go to bed, right?
You need to take a nap. Or, you know, it’s a, a weekend and the student is feeling anxious, you know, and, and, and you can see, hey, you know what your, your, your activity factor is kind of low. What you need is go take a walk or go, you know, go up and down the stairs or go to the gym or something like that, right?
So, contextual person specific, but also using this intelligence to help. Guide positive health behaviors.
Bret:
Yeah. All that sounds so fascinating and so important and really could be incredibly impactful. Well, if people wanted to follow you and learn more about you, where would you direct them to go?
Ryan:
Okay, so I need to get better at it, but, you know, one of the best places is emotional fitness.blog. That’s a, a blog that I have that I’m trying to use to, again, every step that you can take, there’s something you can do to improve your mental health. And helping, people find that unique formula for themselves from a menu of offerings.
Bret:
Great. Well thank you for all your work and thank you for joining me to have this discussion today. I really appreciate it.
Ryan:
Yeah, thanks. It was great meeting you and I appreciate the time here today.
Listen, Watch & Subscribe on:


Youth mental health refers to the emotional, psychological, and cognitive well-being of children, adolescents, and young adults. This period of life is marked by rapid brain development and…
Read more
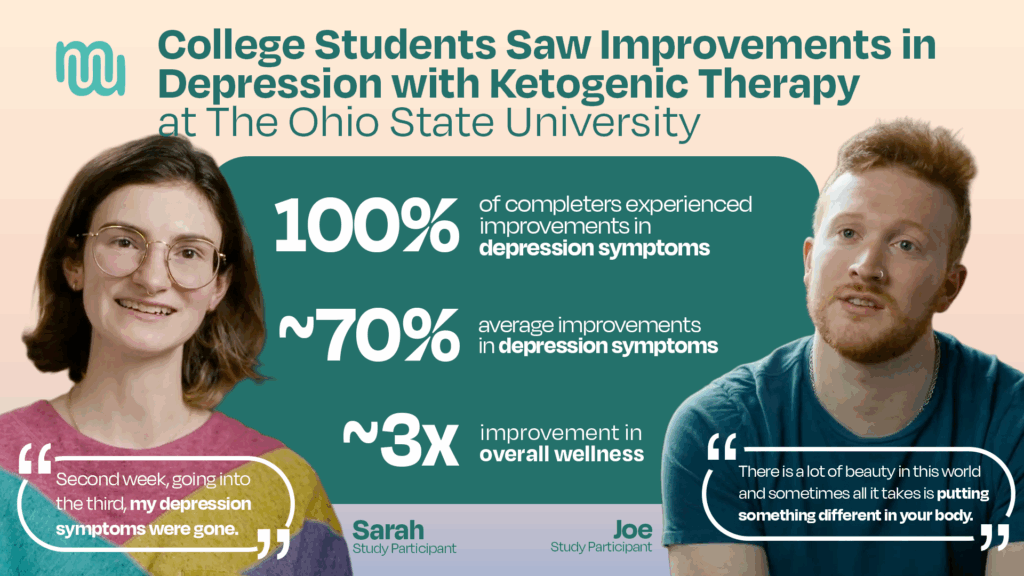
A new study shows an association between at least 10 weeks of following a well-formulated ketogenic diet and a roughly 70% decrease in depression symptoms among a small…
Learn more

The promise of ketogenic therapy for treating mental illness is accelerating with the newly published findings of a pilot study at The Ohio State University, which showed remarkable…
Learn more
Youth mental illness is on the rise, and treatment options are often limited, especially for kids with bipolar disorder. In this interview, Elizabeth Errico, founder of the Children's Mental Health Resource Center (CMHRC), shares how her organization is implementing ketogenic therapy in a real-world setting for kids aged 6 to 17. The year-long study is part of a larger initiative supported by the Baszucki Group to expand mental health care options through metabolic approaches.
Learn more
Youth mental health refers to the emotional, psychological, and cognitive well-being of children, adolescents, and young adults. This period of life is marked by rapid brain development and…
Read more
A new study shows an association between at least 10 weeks of following a well-formulated ketogenic diet and a roughly 70% decrease in depression symptoms among a small…
Learn more
The promise of ketogenic therapy for treating mental illness is accelerating with the newly published findings of a pilot study at The Ohio State University, which showed remarkable…
Learn more
Youth mental illness is on the rise, and treatment options are often limited, especially for kids with bipolar disorder. In this interview, Elizabeth Errico, founder of the Children's Mental Health Resource Center (CMHRC), shares how her organization is implementing ketogenic therapy in a real-world setting for kids aged 6 to 17. The year-long study is part of a larger initiative supported by the Baszucki Group to expand mental health care options through metabolic approaches.
Learn more