New Results: First RCT for Schizophrenia & Bipolar Disorder. Learn more.

Listen, Watch & Subscribe on:



Cholesterol & Heart Health: Insights from LDL Research on Keto with Dave Feldman & Nick Norwitz, PhD
Listen
About the host

About the guest

About the guest

About the host
About the guest
About the guest

Dave:
And indeed there is a huge difference in LDL cholesterol that’s shown to one side. And yet, on the plaque, there’s no statistically significant difference with even a trend in the direction of lower plaque on the keto side.
Bret:
Welcome to the Metabolic Mind Podcast. I’m your host, Dr. Bret Scher. Metabolic Mind is a nonprofit initiative of Baszucki Group where we’re providing information about the intersection of metabolic health and mental health and metabolic therapies, such as nutritional ketosis as therapies for mental illness.
Thank you for joining us. Although our podcast is for informational purposes only and we aren’t giving medical advice, we hope you will learn from our content and it will help facilitate discussions with your healthcare providers to see if you could benefit from exploring the connection between metabolic and mental health.
Engineer Dave Feldman and PhD and medical student Nick Norwitz have published a pretty groundbreaking study that’s making us really rethink how we see LDL cholesterol, heart disease risk, metabolic health, and the intersection of these three components, but also how we see coronary CT angiogram as a diagnostic tool. They’re really turning a lot of paradigms on its head and making us ask deeper questions.
So ,let’s talk to these two authors about how they see the implication of this groundbreaking newspaper.
Dave Feldman, welcome back, of course. And let me start by just saying congratulations now that you’ve got another publication. This one about your lean mass hyper-responder and the Miami Heart Match Study published in JACC: Advances. So, we’ll get into the details, but one after another.
All these publications from an engineer with no research backgrounds as we’ve talked about before. Congratulations. How are you feeling?
Dave:
What can I say? I’m feeling fantastic. You’ve watched the journey from the beginning. So, you’ve seen the story unfold before your eyes.
Bret:
Yeah, and of course, not just you’ve assembled an amazing team with Dr. Matt Budoff and Dr. Adrian Soto-Mota and Dr. Nick Norwitz, and the whole team really deserves a lot of congratulations for getting this out there.
But you’ve been the spearhead from day one. So, let’s talk about the study a little bit and then get into sort of the implications and, the nitty gritty details as I like to do with you.
So, 80 patients from your lean mass hyper-responder, or 80 subjects, I should say, from your lean mass hyper-responder cohort matched with 80 individuals from the Miami Heart. LDL of 123 on average for Miami Heart, LDL of 272 on average for the lean mass hyper-responders matched for age, and metabolic health, and so forth, and looking at their plaque.
Does that set it up about right?
Dave:
Pretty much, yes.
Bret:
Okay. Now, so like you give us the details. What’d you find about these matched cohorts and what the difference or similarities were in terms of their coronary plaque by CT angiogram?
Dave:
That’s what was exciting about this is when we started the lean mass hypers-responders study.
Quite literally ,when I was promoting it for the first time, I didn’t actually think we would have a match. Fortunately, Dr. Khurram Nasir had already initiated the Miami Heart study, and that’s where they collected this cohort that we were able to do a match with. And, indeed, after comparing the CT angiograms between both cohorts, yeah, actually we, you’ve probably seen the other graphs before as presented by Dr. Budoff and myself.
But now we have box plots that actually show it even a little bit better, I think, or at least a little more to people’s understanding, which show that indeed there is a huge difference in LDL cholesterol that’s shown to one side. And yet, on the plaque, there’s no statistically significant difference with even a trend in the direction of lower plaque on the keto side.
But as always, I re-emphasize still no statistically significant difference. I only bring up the trending to bring forward that I think a lot of people would be curious to at least know the trend if those people with much higher LDL, as is the case with our cohort, were indicating that they might break away towards greater plaque, even if not significant yet. And that’s just not what the data show so far.
Bret:
Yeah, and important to note that these individuals have been in ketosis for on average almost five years with LDLs, like we said, of averaging 270 compared to individuals with LDLs of 123. So, for those cohorts to have very similar plaque scores basically tells us for these individuals after five years, roughly five years of exposure, it’s not enough to cause, be causative of increased plaque. Okay, so what does that mean? How do you help instill that to, how we should interpret that, those findings?
Dave:
Yeah, so let’s go. Let’s first kind of set the table a little bit on the lipid hypothesis. You could say there’s two versions of the lipid hypothesis. And that’s the hypothesis that higher LDL is a central driver of plaque development, period.
And the simple version of this hypothesis is it doesn’t matter what the population is. If you have high LDL, you will see a greater development of plaque, full stop. There’s a second category, if you will, of people who say, think that there’s a lot to be said for it, that there may, in fact, be some driving components, but it’s hard to say for sure until we’ve really tested it in all of these various populations to confirm if it really is that simple.
And as this is something I’ve been vocal on for a long time. My concern is that virtually all of the data that we get that show that association between LDL and the development of coronary plaque is from populations that have other things, like insulin resistant syndrome, that independently associate with greater cardiovascular disease separate from lipids, but also themselves impact our lipid profile.
So by definition, it’s a confounder. This is the same, by the way, with genetic abnormalities, such as homozygous familial hypercholesterolaemia. That’s a mouthful. But as you know, that was one of the most compelling cases going back to the work of Brown and Goldstein because this dysfunction in lipid metabolism that people had this genetic disease would both show a higher level of LDL and a higher development of atherosclerosis very early in age.
So, this is a new category, a category of people that have sky high levels of LDL. And what I would propose may turn out to be a functional lipid metabolism. And if that’s the case, then, of course, we should be studying them. We should be checking to see if indeed they fit that first version of lipid hypothesis, which could be applied universally.
And I think right now this is, without question, some of the most compelling data that seems to push back on that simplistic version of the lipid hypothesis.
Bret:
Yeah, I think that’s very well said. Another way to say it is you have to consider who you’re talking about, the LDL, rather than just the LDL itself, right?
The patient matters, the background of the patient and the metabolic health matters. So, we talk about the difference in LDL between the two groups, and there was no difference in plaque score. So, we’ve talked about this before, but very important to clarify. This is coronary CT angiogram, not coronary calcium score.
Because people will say calcium score is a late finding, vascular disease takes decades to develop. But I think you, we can maintain that when you’re using the most sensitive tool, that is not necessarily the case. So, I’m sure you’ve gotten a lot of pushback that four and a half, 4.7 years, five years isn’t enough time for the lifetime exposure of LDL to make a difference.
So how do you counter that?
Dave:
Actually, yes, this does come up a lot. And to that, I bring them back to their own data that they cite back to me. Because again, if you’re looking at it from the simplistic view of LDL and its association with development of coronary plaque is quite straightforward.
So, for example, when I had first shared this with Dr. Rhonda Patrick and Lane Norton, they were both pointing to Mendelian randomization studies. These are studies that look to genetic abnormalities that result in a difference of LDL cholesterol and the corresponding development of atherosclerosis.
It’s usually in the case of lowering, as in for each stepwise lowering, you can see a drop in corresponding risk. Now, the one that they linked, I’d actually ran the numbers on just a couple days ago. And if you look, as you probably already know this yourself, Bret, these changes aren’t even that much in MR studies.
They often can be like, say two to four milligrams per deciliter up to the most, 20 milligrams per deciliter. And that’s in the case of PCSK9 loss of function. If you see the differences between them, the average around 7.5 milligrams per deciliter. And the difference between Miami Heart and our cohort is 149 milligrams per deciliter.
Now, if I’m steelmanning their position, what they would say is, yeah, but this is only 4.7 years and Mendelian randomization is over the lifetime. I agree, but you can add those numbers together to find out for yourself. And I can tell you from the Mendelian randomization study that they linked, the largest distance between two of the different SNPs, two of the different genetic abnormalities that result in the biggest difference in LDL.
If you add those together over the lifespan of, say, somebody who is an average of 77 years old, which is the average of an American, you multiply times 77, you end up with a little over 700 milligrams per deciliter. So, a difference of over 700 milligrams per deciliter over the lifetime should show a clear signal of coronary heart disease risk.
Guess what? 4.7 times 149 is just over 700 milligrams per deciliter. So, Bret, we should absolutely, using their math, using the math, the Mendelian randomization, we should absolutely see a signal of plaque development and progression, and I just don’t think the data supports that so far.
Bret:
And I like how you said, so far. We have what we have, right?
And it’s the first of its kind. So, it’s not going to be the last word, and the end all, be all. But it is the first word and a very exciting sort of look at this. This is a way of thinking about this that we haven’t before and probably should based on the data. Now, people may take that to say, see, this answers the question.
This falsifies the lipid hypothesis. This proves LDL has nothing to do with heart disease. How do you respond to those claims based on this data?
Dave:
Yeah, of course. I then take us back to these two categories, right? Does this seem to have the strongest data to date that pushes back on the simplistic version of lipid hypothesis?
To me, I think it does. It absolutely provides the strongest data to date. Would I say it’s definitive? No, I would not. And I think all of my co-authors would agree with me on that. I don’t speak for them, but I’m pretty sure that they would agree with me on that. Now, a more complex version is, I think, worthy of mentioning, which is many people, and I don’t want to speak for you, Bret, but you and I have had these conversations.
I think there’s an emerging number of doctors who say, I’m not ready to believe the lipid hypothesis is too small of an affair to consider in the case of patients who don’t just have high LDL, but they also have other cardiovascular risk factors. There may be more to the story there.
And to which case, I want to emphasize that indeed what we’re looking at are populations that have low to no cardiovascular risk factors in the beginning. And I’m more than happy to expand on that nuance and make clear that’s exactly what we’re looking at. So, this more nuanced version of the lipid hypothesis I want to acknowledge is something that’s getting looked at and should get looked at.
But many, like yourself, now have a sort of a checklist that I talked about in my last discussion, which goes like this. If a patient comes into your office, and they have high LDL. Let’s say they went on a ketogenic diet, they’re saying, doc, I feel great, but I guess I have high LDL. I, myself, don’t want to, it’s like their wish, I, myself, I don’t want to lower my LDL.
Is there something more we can do to better find out where I stand with risk? And many like yourself, like Dr. Budoff, like Adrian Soto-Mota, they will say, let’s go ahead and get imaging. They would recommend either getting a CAC, or, of course, the gold standard being CT angiography, which we used in this study.
If you’re still low to no risk, then there’s more and more doctors that are emerging saying, okay, if it’s your wish to not take steps, given the existing prognostic power of actually looking at the plaque in your coronary arteries, these data along with existing data, not just ours but existing data that show how prognostic imaging is towards future cardiac events, they tend to be more comfortable allowing for even the levels of LDL that we have in our study now.
I’ll emphasize as I’m sure you’ll want me to, and as you would as well, this isn’t medical advice. Please work with your doctor. This is just what I am observing of a lot of medical professionals out there. My job is not to provide medical advice. I’m just trying to get this research. But it is worth noting that is something that we’re watching change in real time, and I’m happy that this data can help inform people on their decisions with their own doctor.
Bret:
Yeah, and I think we’ve talked about this before. But as much as you could say the star of the study is the concept of lean mass hyper-responder, the co-star is the CT angiogram to show the importance of a test with that level of sensitivity, and early detection of disease rather than studies that are late detection disease.
So, I hope people walk away from this study thinking, okay, we need to think separately about lean mass hyper-responders and metabolic health, but we also need to realize the important role of CT angiogram can play. Now, I think we’re a long way away from insurance companies covering CT angiograms in this setting. But my goodness, it makes the case that maybe we should be doing this if we really want to know about somebody’s risk, and whether somebody’s developing plaque with their high LDL because of their lifestyle that then has other benefits.
I know you’ve worked very closely with Dr. Matt Budoff, who has been a pioneer in CT angiography and calcium scoring. Do you and he share the same enthusiasm about what this study does for CT  angiography?
Dave:
I think we do. It’s fascinating. He is very much an imaging guy. He was working against a controversy 30 years ago in what was called then the mammogram of the heart, which is a coronary artery calcification scan. It’s funny to hear this today because here in 2024, I’ve never been more bullish for a CAC, not because it’s as good as a CT angiogram, but because it does tend to be very correlative.
So, even though you are looking at calcification, and to what you said a little bit earlier, even though it is picking up often what might be considered later stages of disease, I will explain what I mean by that in a moment, its correlation is so close that if you don’t want to go through the invasiveness of a CT angiogram, for example, you don’t want to have the contrast dye.
Or even for the lower dosage for CT angiogram, it’s five times that of a CAC. A CAC is now super cheap to get, and it’s very low dose for radiation. Back 30 years ago, it was a higher dose of radiation but not by that much. And both Dr. Budoff and Arthur Agatston were both looking at it, they were saying, there’s just a no brainer.
This is so prognostic, it’s so predictive of future events. This is going to get widespread approval. So, in that vein, Dr. Budoff is no stranger to controversy for something that was very groundbreaking then, and only now is actually getting adopted, which is part of why I think he’s been a great partner for us in the science.
Yes, he’s been excited, but at the same time, I think he’s a true scientist in that he’s always looking for the next amount of data to build on and the next amount of data to build on. There’s not a point in time where he feels he’s ever done with the thing that he is looking at. He’s always interested in expanding on more.
Bret:
Yeah, I think that’s a great point about how it’s been a 30 year sort of journey to get CACs to be mainstream, and maybe it’ll be the same for CT angiograms. But great point that the CACs, the calcium scores, the radiation dose has come down a little bit, but the CT angiograms, the radiation dose has come down a ton.
I mean from like 15 to 20 millisieverts now down to 2, 3, 4 millisieverts, depending on the individual. And millisieverts is just the measurement. But that’s a tremendous decrease where 15, 20 years ago, we would never consider doing it routinely as a primary preventative strategy.
Yeah, but now we could, and I think that’s something that the study really brings to light. But one other part about this study, so we talk about the LDL. Vast difference in LDL 272 versus 123, but HDL 90 in the lean mass hyper-responders, 63 in the Miami Heart, which is still pretty good for general population, 63 triglyceride, 64 lean mass hyper-responders, 96 in the Miami Heart.
So, definite differences. And body mass index also slightly different, like 22 versus 25. Could people also point out, okay, maybe it’s not just the LDL, but maybe it’s the HDL triglycerides body mass index that also plays into this?
And if that’s the case, does it really matter? Or is that just even more evidence about this special and unique physiologic state?
Dave:
I invite those kinds of comments because if there’s, look to the exact point that you were making. If you’ve got a population of people with an HDL of 60, it’s actually considered currently by modern lipidology, it’s considered to be worse if they went from say a 60 HDL to say a 90 HDL higher.
It’s thought to be that there’s not just diminishing returns, but actually a net detriment the higher and higher your HDL goes. So, that’s one. Triglycerides are considered to be excellent if they’re below 150 milligrams per deciliter. And so even that difference between 60 and 90 is not considered to be meaningful for most clinicians, certainly not something that they would comment on.
Now, the BMI is ,I think, a little bit more interesting and relevant to bring forward. But given this lipid profile, you may know this as a doctor yourself, if they already have a very strong HDL to triglyceride ratio, which both cohorts do, then typically speaking, they don’t have a higher composition of body fat compared to body muscle.
Typically, they’re going to look more like Tom Cruise, who technically has a BMI of 26, or say Joe Rogan or say Arnold Schwarzenegger, who has a very high BMI. They tend to, if they’re in better metabolic health, they tend to have the kind of lipid profiles we’re looking at. Now that said, take any of these three or all three of them together, if you were to say, hey, I think going from a BMI of 28.5 to 22.5 would be extremely protective towards development of atherosclerosis so much that you would completely wipe out the risk level of an additional 149 milligrams per deciliter increase that you see with our cohort versus Miami Heart.
I welcome that discussion. It’s just not what I see in the published literature. I don’t see a case that’s made. Certainly, I’ll bet, since you’ve read, you read a lot of these papers, how often do you see them utilizing BMI and trying to control for the enormous cardiovascular benefit of BMI that’s actually under 26? I, myself, don’t typically see that.
Bret:
Once you get down to that level, it’s assumed that it’s all like normal. And therefore, it doesn’t necessarily need to be controlled for. So, that’s a really good point. I want to address a couple things about that though that with the HDL increase that is thought to be more of a detriment.
That comes from more, I think, genetic studies where people have a genetic predisposition to have HDLs of a 100, 120, and it tends to be less well-functioning or non-functioning HDL. So, I think this also provides a really unique perspective when you get there by lifestyle and dietary interventions and metabolic health interventions and not genetics.
It changes everything. So, it’s not likely a detriment at that level when you get there by what you’re eating and the way you’re living your life. And then the second
Dave:
Exactly.
Bret:
Oh, sorry.
Dave:
Can I just add, please, also alcoholism?
Bret:
Yeah.
Dave:
Alcoholism can also drive up your HDL to an unusually high levels, but that also ties back into exactly what you’re drawing into, which is how much is the reason for the lipid value.
How much is that the actual underlying causative contributor to the net detriment?
And sorry, continue with your second point.
Bret:
No, the way you phrased that summed it up perfectly because that’s the same discussion we’re having for the LDL. Why is the LDL elevated? Why is the HDL what it is?
And then for the triglycerides, like you said, if normal quote unquote, and I got to put those in really ugly air quotes, is 150. But maybe now your study is saying, eh, maybe normal is 60, maybe normal is 75, right? Maybe we need to redefine what normal is? So, I think there are a lot of things you can pick out of these results that, of course, need to be expanded upon in future studies.
But I think it contributes so much more than just the high LDL, the lean mass hyper-responder. But as you break down to the specifics of what we define as normal and metabolically healthy, so do you think there will be more to come based on this study from those specific elements?
Dave:
There will be from us. One of the, listen, Bret, you’ve watched me put an enormous amount of time and effort into this for the last seven, eight years, and I want to re-emphasize the point you made earlier without question. It’s not just me. I’m highly reliant on a team of amazing people as well as the participants themselves to make this happen, to make this a reality.
But as of this moment, as of this recording, I can’t say that I’m aware of a single other study that’s taking place with a metabolically healthy cohort like lean mass hyper-responders with extremely high levels of LDL. In this context where we can actually observe them, we can look at the high LDL and high ApoB absent other things that are known to be confounders for cardiovascular disease, such as dysfunction and lipid metabolism, and I think that’s unfortunate.
I really do hope that this research helps to propel, compel more and more people, especially those who literally research this for a living to look into why this phenomenon is so relevant. And my hope is this data, this data from this study will spark more interest for more and more teams to want to find out what’s going on under the hood.
Bret:
Yeah, that’s a, that’s such a great way to say it. And the fact that it was published in a sub-journal of Journal American College of Cardiology, so JACC: Advances. It is going to get so much attention, and I hope people are going to say, huh, I want to look into this more exactly like you’re saying.
And clinicians will hopefully say, huh, maybe I need to think more about metabolic health and about triglycerides and HDL and using CT angiograms? There’s so much people can start to take away from this and start to think about how to explore more for the individual patient and from a research side.
And then, of course, we have more coming from you and your team. So, now that we’ve got this publication, which is super exciting in its own right. What can we expect in the near future from you and your team as well?
Dave:
I can tell you we’ve got some great mechanistic studies going on the mechanistic side of the fence, but with regard to risk, we actually have the quantified data that’s coming soon.
So, everything you’ve seen up until now is assessing the plaque with what’s known as a TPS or total plaque score, and that’s using a human reader like say, Dr. Budoff, going through these CT angiograms in 3D, going to the different sites of interest and giving them a score. And that’s based on his expertise.
No question. But where this gets really interesting is where you run it through something like Cleerly. Cleerly does a quantification analysis where an AI-guided reader, which also can get to, which can also get to greater levels of resolution. So, they can look in a bit tighter, actually quantifies the plaque. And spoiler alert, in their scans, everybody has plaque because everybody does have plaque.
It’s kind of all of us have cancer, right? It just depends on how tight a resolution you can get down there because, eventually, you’ll find that we all have cancer cells to some degree. By that same token, this becomes important because then we need that for being able to do the longitudinal analysis.
Looking at scans from day zero. To the scans one year later for our cohort so that we can do what’s known as a longitudinal analysis. And that’ll be the LA last major paper of, I’ll say this phase, and I’m saying this phase because what’s great is that we collected a lot more data than we technically needed for the longitudinal analysis.
You may already be familiar, but for example, we captured Lp(a) that may end up being coming its own paper. We also will be doing a much more thorough analysis on the particles themselves. I’m not even just talking in NMR, which breaks out the different variations of the particles, but actually using something like Nightingale, which we’ll get into the composition of the particles themselves, including LDL particles.
You’ve heard me make this prediction a million times before, but I’m going to make it one more time. I believe lean mass hyper-responders are going to actually demonstrate that they have a difference in the composition of their particles compared to say somebody with the same size particles but who’s metabolically challenged.
And that gets to that larger question you were talking about earlier. And that’s so, is of such enormous importance to me, which is the heart of causality itself. The simple version, the simple version being, it doesn’t matter what the reason is if it’s higher, it’s worse. That does suggest independent causality.
If the reason for why something is high doesn’t matter that much, then we relate it to something like smoking. Doesn’t matter if you’re the one who smoked the cigarettes, if you’re in a bar where you get the exposure of smoke that’s equivalent to three packs a day, you’re still at a very high risk. Even if there’s a slight modulator here and there, doesn’t matter.
It’s the central driver, right? We want to know the same thing about ApoB lipoproteins, like LDL. Will it be a central driver with people who have levels as high as 272 or as high as my colleague, Nick Norwitz, who’s up there in the five hundreds? I mean, obviously, I’m hoping he’s not at the same level of risk, but time will tell as we collect more and more of these data.
Bret:
And you mentioned Nick Norwitz. I’m excited to have him, to get his perspective on this as well, which is who we will talk to next. But I want to thank you for all your contributions, and all your hard work to start this, your dream. It started many years ago, and to see it come to fruition with multiple publications and more to come, really helping change the face of how we see LDL, how we see metabolic health and how we realize we have to evaluate people individually.
So, thank you for your contribution.
Dave:
And thank you, once again for having me, Bret.
Bret:
All right. Nick. We just heard from Dave Feldman. We’ve heard a lot about this paper, and it’s pretty monumental to have it published in something like JACC, a JACC: Journals, which is very mainstream cardiology. So, I’m curious about your experience though. You have a very unique experience as a medical student.
So, first of all, like a huge honor of how you’ve published so many papers as a medical student, but papers that sort of go against the common teaching, common belief, common paradigm, which as a medical student could be a little dicey. So, I’m curious to get your perspective, how you feel from the inside of the institution, so to speak, publishing papers that go against what you’re being taught.
Nick:
I’ll frame this just with respect to my anxieties even going into med school because I always knew I was a little bit different in my perspective, given my background. So, I remember going into med school, I wrote a piece for STAT, just like a science arm of the Boston Globe, saying will a ketogenic diet made me a pariah in medical school?
And to my surprise, I found that’s not at all the case. Like when you’re boots on the ground with other just genuinely curious intellectuals. People tend to have their guards down and be very open-minded to new data, which is really interesting, for me, being someone who is a scientist, is a medical student and is also involved in the social media world. Because I get to see that juxtaposition of the social media and the behavior of academics on social media versus their behavior when you are in academic settings.
It could not be more distinct. Probably that’s in part because of what people tend to spend a lot of time on social media versus who don’t. But I also think it’s a phenomenon of people watching people, or academics realizing they’re on display for the lay public, where they may want to have a more conservative message because they’re really concerned, right?
First, do no harm about people taking an inch and turning into a mile, whatever the expression is. I’m framing it out. But behind closed doors, I find universally when new data come up like this that are appropriately caveated, which if you actually read the text, we caveat tremendously and just asking sincere questions.
People are just interested because the data are the data. And you can say, these are new data, they rub against the grain of a conventional approach. But we all know in our hearts that like what we’re learning now about half of it’s wrong and we’re open to the idea that the half that we’re attached to might be wrong.
And that’s, I feel like in academic settings seen is a little bit more thrilling, and in public settings a little bit scarier. I’ve thought a lot about why that might be, why there’s that distinction in behavior. I think what I’ve come to is it’s easy in an academic setting to parse the clinical from the scientific.
Say here are new ideas, new models, and we can talk about them as such in the abstract versus in the clinical setting. You’re like thinking about how is a patient or a person going to take this information and enact it right now? And those things on social media tend to blend. So, when I ask a question like, do we know that lean mass hyper-responders with super high LDL and ketogenic diets are at increased risk?
The fact of the matter is that is a totally legitimate question to ask and is not at all the same as the statement, which this keeps on, I keep getting taken out of context. So, we’ll see if this happens again.
But were I just saying, which I’m not saying, LMHR aren’t increased risk. There was a recent episode, you can ask Dave about it, but somebody just took what I said, literally where that context where I was like, I do not believe X, Y, Z. And they’re like, ah, Nick said X, Y, Z. See, there’s the question, and there’s the statement.
And if you are an academic, I think people understand like how you could see the distinction. But in the public setting, people get very nervous, or I think clinicians and academics get very nervous about how the general public might take it. And I think it’s that blending of the scientific and the clinical that creates, not the facade of controversy, but unnecessary controversy in social media.
Bottom line, because I like to spiel, I find in academia versus social media, there is a lot of open-minded acceptance, which is great.
Bret:
Yeah, such a interesting juxtaposition. The discussion you can have with open-minded, curious individuals versus the sort of knee-jerk reaction on social media, which are just two completely different worlds. But it’s the world we live in, so we have to acknowledge that people are going to see this study. And in social media posts on this study, and they may walk away with a thought, oh. I don’t have to worry about LDL.
It doesn’t mean anything. And even though you caveat like crazy with your papers and your posts, someone can still walk away with that. And then, the clinician who sees that paper is going to be like, ugh, that Nick Norwitz, he’s telling people that LDL is fine. So, there is this snowball effects. So, I don’t even know where I’m going with this other than to acknowledge it and say like, how do you like wrestle with that to say okay, maybe some people are going to get the wrong idea because of what I did, but I can only do what I can do to try and give the right message?
Nick:
I have a kind of poking, controversial take on this. I’ve thought about it a lot. And on the one hand, you can see the binary as, okay, I’m going to put out information that’s legitimate, but there is a risk involved. And that is fully my responsibility and my team’s responsibility as those who are doing the research.
I don’t have that perspective. My perspective is that it’s the responsibility of the academic community on social media to accurately represent what’s being said and what’s not being said. And I think confusion arises when other academics, straw men are positions and say things that we don’t actually say or aren’t willing to platform nuance.
I think there’s a perspective probably more around Dave than myself, but that he’s a quote, dangerous person to platform, and I think that is exactly opposite of reality. I think what we need to do is have across the aisle discussions. Nuanced conversations about the caveat, so you can hear from the researcher’s mouth what we’re actually saying, rather than the caricatures that get created by detractors.
Because quite honestly, keto bashing is a great tool for getting social media engagement. We’re talking about acknowledging facts here. That’s one fact. And so we often find that our group in our research gets straw manned, and our positions don’t get fairly represented by others. Sometimes, apparently intentionally, even after like behind the scenes, we’ve had long discussions with these people, they’ll go on and present things that we didn’t even say.
So, it’s difficult. What I would say is I try carefully to reflect on my messaging what people are sincerely taking away from it, and try to correct the record where others misrepresent our perspectives. Then there’s the other level, and this is a little bit more difficult, trying to assess where somebody’s actually led astray versus where someone is just engaging in confirmation bias.
Oreo versus Statin was a great example because I knew it would happen. I knew somebody, people would be saying, Nick’s saying LDL isn’t harmful, which I never said. Or Nick’s saying, LDL, I mean statins don’t work. I’m like, they had the exact expected effect you would. The Oreos just were, had a more profound effect in this context.
People were always going to make those claims. I was prepared for that, but I also knew that people that were going to make those claims already had that perspective and were doing mental gymnastics to use our data or our presentations for their own aim. So, I don’t actually think minds were changed. It was just pre-existing confirmation bias and people saying their piece, which happens all the time.
I don’t actually see that as an active harm. I don’t know what your take is, or maybe I’m just being disingenuous and trying to defer responsibility?
Bret:
No, I think that’s a great perspective, and I think it’s a really important perspective. But let me ask you one last question here about this.
So, you are in medical school at Harvard. So, you know people can come and talk to you specifically about this paper, and you can really educate from the inside out. But there are hundreds of medical schools across the country, across the world. What do you hope medical students in those institutions and their attendings will read your paper and walk away, and what do you hope they will take away from it? And what do you hope they will change today based on the papers, on the results?
Nick:
I’ll first represent something that was unexpected from the Oreo versus Statin just because I think there actually is direct clinical relevance. This is something I’ve talked to you about before, but then I’ll talk about the scientific and the abstract. But the work we’re doing speaks to a unique population. Lean mass hyper-responders, which while people could say it’s a small population, it’s growing really rapidly as ketogenic diets become more popular and more people are using them for more use cases.
So, understanding the existence of this phenotype now. The model, the lipid energy model behind it, has direct clinical relevancy insofar as understanding the physiology allows you to trial experimental protocols that could potentially attenuate risk in these patients. So, I say this in the face of the data that you’ve now just talked about with Dave and are talking about with me, where we didn’t find in these preliminary data increased plaque in the lean mass hyper-responders. However, that’s not the end of the story.
It’s only the beginning. So, we still might, or we do have LMHR patients who want to lower the LDL because the data are still developing. And by being aware and engaging with these literature, clinicians and clinicians to be, can try personalized approaches to risk attenuation, which for some and many lean mass hyper-responders who can afford to have some carbohydrates, could be sweet potato therapy or fruit bowl therapy with twice the efficacy of Crestor.
And so I bring this up because it was an unexpected result of the Oreo versus Statin where I was getting cardiologists reaching out to me like, because I went down the rabbit hole on this literature, because I was aware of it from these published papers. I’m now treating my patients instead of with statins with various carbohydrate titration protocols based on their unique clinical setting.
And both they are and I, I being the clinician, are very happy with the results. So, I think there is direct clinical application today. But beyond that, I’m just excited as a scientist kind of separate from the clinical about these data and what they could mean for our understanding of human physiology.
While I don’t think that the guidelines, standard of care will change overnight, nor should it, I would, not that they need permission, but give permission to the medical students, the residents, the clinicians to actually just get excited about engaging in the process of science and seeing how things develop.
And if that just means sitting on the edge of your seat with some popcorn and being in tune with the research and having academic discussions and being open-minded and not changing your clinical treatment paradigms with your patients at all, that’s fine. But I think that actually sets the groundwork for productive discussions that in the long run, and the long arc of science and medicine, do and will help people.
Bret:
Yeah, such a good answer. Yeah. As I was, I asked the question, I was thinking of the answer, too. And I think it would be risky for a medical student to jump on this and say, this is how they’re going to treat their patients and so forth and make changes. But such a strong, powerful lesson to say this is how you ask questions, and this is how you explore those questions, whether it fits the paradigm or not.
If you’ve got a reason to question it, then ask the question and explore it. And that’s what you’ve done a fabulous job. You and Dave and Dr. Budoff and Dr. Soto-Mota and your whole team have really done an amazing job of showing how to respectfully and in a sound scientific way, ask the question and follow through.
So I, for one, am very grateful for doing that, and I definitely look forward to hearing more as we get more information about this cohort and future publications. So, thank you.
Nick:
Thank you so much, Bret.
Bret:
Thanks for listening to the Metabolic Mind Podcast. If you found this episode helpful, please leave a rating and comment as we’d love to hear from you.
And please click the subscribe button so you won’t miss any of our future episodes. And you can see full video episodes on our YouTube page at Metabolic Mind. Lastly, if you know someone who may benefit from this information, please share it as our goal is to spread this information to help as many people as possible.
Thanks again for listening, and we’ll see you here next time at The Metabolic Mind Podcast.
Listen, Watch & Subscribe on:

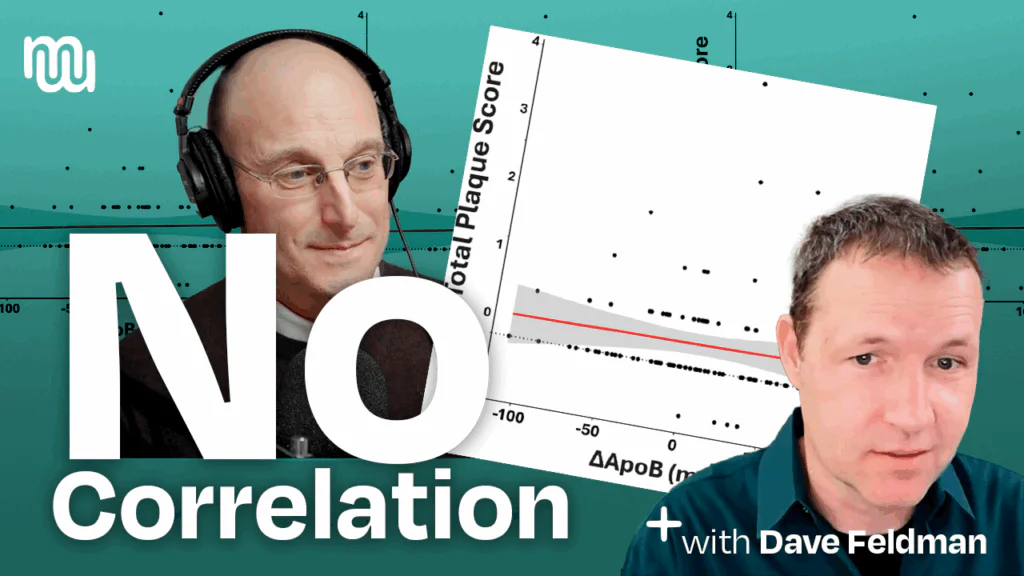
Engineer-researcher Dave Feldman walks through the lean-mass hyper-responder (LMHR) keto-CTA trial: 100 metabolically healthy keto eaters with very high LDL/ApoB had coronary CT angiograms at baseline and ~1 year. Key finding: changes in plaque (including non-calcified plaque) did not correlate with LDL or ApoB; the best predictor of progression was pre-existing plaque. Keto itself wasn’t shown to drive plaque, and saturated-fat intake and cumulative on-diet LDL exposure didn’t track with ApoB or plaque change either. Plaque did rise modestly for some—about what’s seen in treated cohorts—while a few even regressed; interpretation should be individualized with imaging (CAC/CTA) guiding care and standard therapies used when plaque is present. Limitations (e.g., no longitudinal control group) mean more studies are needed; Dave’s team is launching follow-ups and invites open, civil debate—“don’t confuse arsonists with firefighters.” Resources: CitizenScienceFoundation.org and cholesterolcodemovie.com.
Read more

Have you wondered if there is a better way to predict the risk for heart disease than using LDL cholesterol? It turns out, there is. Discover why coronary…
Learn more

Why should we rely on a blood test to assess heart disease risk when we can see the disease itself? Transcript: Introduction to Carotid Intima-Media Thickness test (CIMT).Have…
Learn more
A one-year prospective study found that very high cholesterol in 100 otherwise metabolically healthy individuals on a ketogenic diet for an average of 5 years did not correlate…
Learn more
Engineer-researcher Dave Feldman walks through the lean-mass hyper-responder (LMHR) keto-CTA trial: 100 metabolically healthy keto eaters with very high LDL/ApoB had coronary CT angiograms at baseline and ~1 year. Key finding: changes in plaque (including non-calcified plaque) did not correlate with LDL or ApoB; the best predictor of progression was pre-existing plaque. Keto itself wasn’t shown to drive plaque, and saturated-fat intake and cumulative on-diet LDL exposure didn’t track with ApoB or plaque change either. Plaque did rise modestly for some—about what’s seen in treated cohorts—while a few even regressed; interpretation should be individualized with imaging (CAC/CTA) guiding care and standard therapies used when plaque is present. Limitations (e.g., no longitudinal control group) mean more studies are needed; Dave’s team is launching follow-ups and invites open, civil debate—“don’t confuse arsonists with firefighters.” Resources: CitizenScienceFoundation.org and cholesterolcodemovie.com.
Read more
Have you wondered if there is a better way to predict the risk for heart disease than using LDL cholesterol? It turns out, there is. Discover why coronary…
Learn more
Why should we rely on a blood test to assess heart disease risk when we can see the disease itself? Transcript: Introduction to Carotid Intima-Media Thickness test (CIMT).Have…
Learn more
A one-year prospective study found that very high cholesterol in 100 otherwise metabolically healthy individuals on a ketogenic diet for an average of 5 years did not correlate…
Learn more