Professor Matt Budoff responds to questions about the new study on Keto, Cholesterol and Plaque Progression
There has been a lot of discussion about the new Keto-CTA study looking at LDL cholesterol, ApoB, plaque progression and cardiovascular risk in Lean-Mass Hyper-Responders (LMHR) on keto.
Two of the biggest misconceptions we have heard are:
- ❌ This study shows that keto causes rapid plaque progression ➡️ Not True
- ❌ This study shows that keto causes rapid plaque progression ➡️ Not True
Over the weekend, we hosted the study’s lead investigator, Dr. Matthew Budoff from UCLA’s Lundquist Institute, on the Metabolic Mind Podcast to discuss some questions that have surfaced about the study. The transcript of the conversation follows.
Keto-CTA Study Confusion: Addressing the Misunderstandings with Dr. Budoff
Dr. Scher: Welcome Professor Budoff. We just posted the video where you discussed the results of the Keto-CTA study focusing on Lean Mass Hyper Responders and the coronary CT angiogram. There’s been a lot of discussion about it, which is great. Anytime you put out novel research, it should stimulate some discussion. But I think there’s been a lot of misunderstanding, misrepresentation, and just confusion about what a lot of the results mean, specifically the CT results. You’re one of the world’s experts in CT angiograms, and you’ve been studying this for such a long time. I think it’s great to have you come back on to help us clarify what these results really mean and what we’re even measuring. So for starters, can you define PAV? Because one of the big questions is that supplemental table showing the change in PAV, but I think a lot of us don’t even really understand PAV. So let’s start from the basics.
Dr. Budoff: PAV stands for Plaque Arthroma Volume. When you calculate it as a percent, that means that you’re calculating it as a percent of the total volume of artery measured. The reason we measure it in that way, PAV percent, is because a lot of the early data came from intravascular ultrasound where they only measured one or two segments of the artery. On CT angiography, we can measure all of the coronary trees. So the amount of volume measured is much higher. You don’t want to just know how much plaque there is, but how much plaque there is relative to the amount of arteries that you’re measuring. That’s why we use PAV percent as a primary endpoint in many trials, because it’s translatable to all of the interventional work that’s been done over the past 20 or 30 years.
Dr. Scher: I’m glad you brought that up because a lot of the CT angiogram studies are relatively new. Whereas the past couple of decades, we’d put a catheter in somebody’s artery, actually in the artery itself to do an ultrasound from the middle of the artery, which now we can do this noninvasively so, would you say with PAV, those studies are relatively translatable such that we can compare one to the other?
Dr. Budoff: Well, if you use PAV percent, you certainly can. There are still some differences. The intravascular ultrasound people only look at certain plaques, certain types of plaques, whereas we looked at all types of plaques. So there are still some intrinsic differences, but I think it does help give us a more broad understanding of what we’re seeing. We can also compare it to other interventions that haven’t yet been done with CT, that have been done with intravascular ultrasound. So it kind of opens the door for a broader look at our results.
Dr. Scher: That’s very interesting. Now that we have a background of PAV, is it safe to say the analogy is you take the house and you have your total square foot of the house, say 2000 square feet, and there are 200 square feet of mold in the house. Then you would calculate your PAV as 10%. Is that a good analogy?
Dr. Budoff: Exactly! But if you had a huge house, it would only be 1%, and it would not be nearly as dangerous. That’s where we’d like to look at percent PAV because it depends on how much of what you’re measuring compared to how much is present overall in the patient.
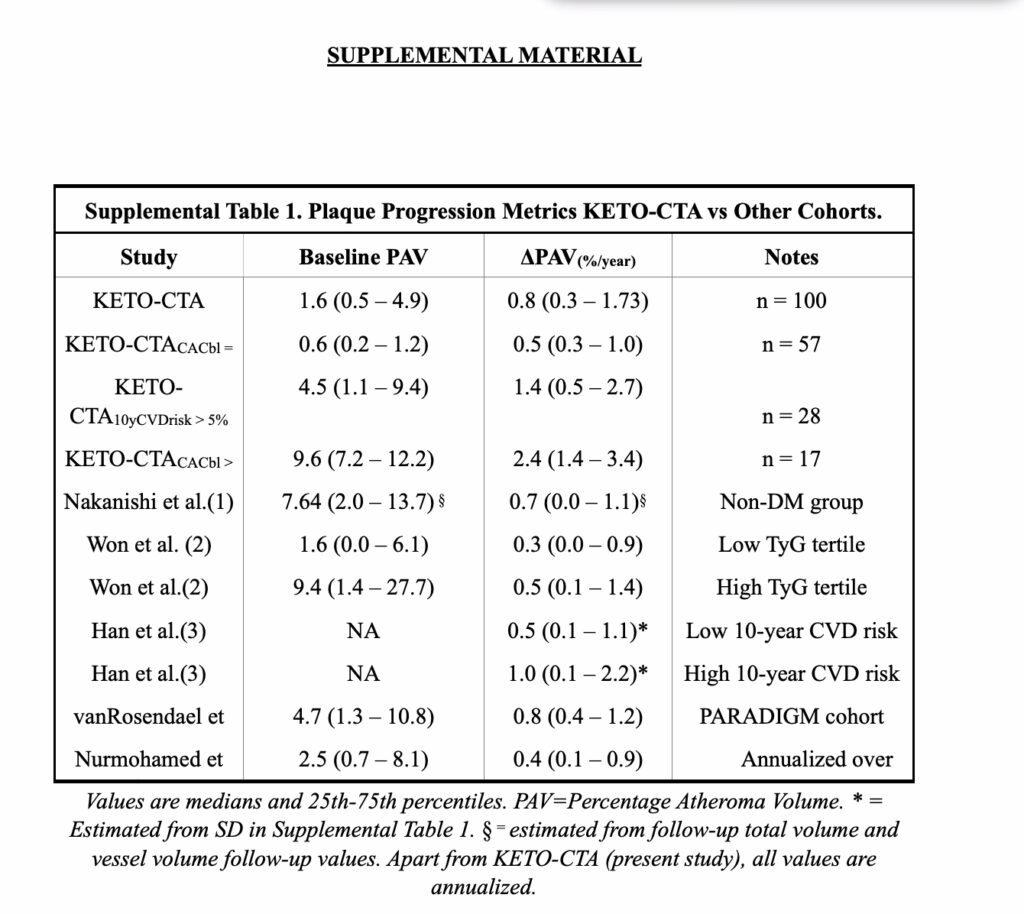
Dr. Scher: So now if we look at supplemental table one from the Keto-CTA study, and we look at the all comers, the baseline PAV is 1.6 and the Delta PAV is 0.8, and that’s for all 100 participants. Some people are interpreting that as saying that is a 50% relative increase, which is higher than any trial has ever shown and is incredibly concerning. If you look at the numbers, they are correct. It is a 50% relative percentage increase. So how do you interpret that type of change?
Dr. Budoff: Well, one, you can’t do it based on a percent because the denominator was very low. The denominator was lower than most other trials. When you have a low denominator, any number looks big. For example, if I tell you that you had a calcium score of one, and it went up to a calcium score of three, you might say that’s great. One and three are both very low calcium scores. And therefore I’m in great shape and over two years or one year, that was a minimal change. But if you calculate a percent change, that’s 200%. And if I tell you your plaque is going up by 200% in one or two years, you might be panicked. But that’s a misinterpretation of the data.
We don’t calculate a PAV percentage change over time, because the denominators are so important when you think about those things. The other thing that you have to remember with the keto study is that we took in patients who were across all types of plaque, but were on no other medical therapies. They weren’t on antihypertensives and they weren’t on statins and they weren’t on anti-inflammatories or aspirin. We took a natural history, a treatment-naive population, and we said: “What is the effect of a high LDL-C on plaque progression induced by the keto diet?” We found that it was not related to the LDL. That is the answer to the important question we were asking.
The question of whether some of these patients who had a lot of plaque should be on a statin, or other therapies, to slow down plaque progression, is a whole separate question. And we have recommended that they go on other therapies once we identified them as having plaque. But this was a true treatment-naive population that was using a keto diet for overall health. And we thought that they were all lean, healthy people. Some of them had a lot of plaque at baseline, which to me was, I think, a difference between the other studies. All the other comparator studies used two, three, four, five background therapies to treat patients. You can’t say a treatment-naive population progressed more than a treated population and be surprised; that’s just too naive to even think about.
Dr. Scher: That’s a really good point. It also speaks to the fact that Lean Mass Hyper Responders are not all the same. There are some who are going to be lower risk, some who are going to be higher risk, and plaque definitely did progress in those patients. But as you’re saying, the study did not suggest that it was due to the LDL. There are other reasons for plaque progression.
Let’s talk about the absolute plaque progression. Those who had a baseline calcium score of zero had a very low PAV of 0.6, which is much lower than any of the other comparator studies, and then increased by 0.5. So what does an absolute delta PAV of 0.5 mean in that context? How do you put that into perspective?
Dr. Budoff: So 0.5 is what we achieve on treated populations. If you look at that supplemental table one, we didn’t include the interventions. But these are populations of patients that were largely on statins or on other lipid lowering and antihypertensive therapies. We achieved a PAV of just 0.5 in some of these populations. So the 0.5 and even the 0.8, in the overall trial, represents similar results to an “on treatment” population of patients who are being treated with multiple therapies. The fact that they only went up by 0.5 or 0.8 on no background therapies at all is actually quite good. And I think reassuring that yes, some of them had plaque and some of them need to be treated. And those that are progressing more rapidly should be treated with other therapies. I think the keto diet is wonderful for a lot of good health reasons. But there are many things that drive atherosclerosis in our bodies, and you can’t address all of them with any one intervention. Some of these patients need to be treated for other atherosclerotic risk factors.
Dr. Scher: Part of the issue with comparing to other studies is that we don’t do a lot of studies on normal healthy people with CT angiograms. That’s sort of a rare thing. Is it safe to say that it is expected that even normal healthy people without other comorbidities, who have high risk, will progress with plaque when you’re using the sensitive measurement such as Cleerly and PAV? Is it normal to expect some progression?
Dr. Budoff: We actually have done that analysis. Remember we compared the keto population, a healthy, asymptomatic population, to the Miami Heart Study, also a healthy, asymptomatic population. We showed there’s no difference between these two groups. Now, we didn’t have progression in the Miami Heart Study, but we’ve already established that these patients were very similar to another cohort of healthy, asymptomatic people. And you’re right. None of the other plaque progression trials ever done have been done in healthy, asymptomatic people. That’s not who we typically study in medicine because that’s not the study group of interest for most of our interventions.
Dr. Scher: Now, I want to get back to the Miami Heart in a second, but just to finish up on the supplemental table, you also show those who have a calcium score greater than 100, which sort of ran from 100 up to even higher than 400 in that range. There were only 17 individuals, but they had a pretty big Delta PAV of 2.4, where I think in general, anything greater than one is considered higher risk. So small numbers with 17 people and they all had calcium scores above 100. So how do you interpret that when compared to, again, some of the other studies which showed lower progression for the entire cohort?
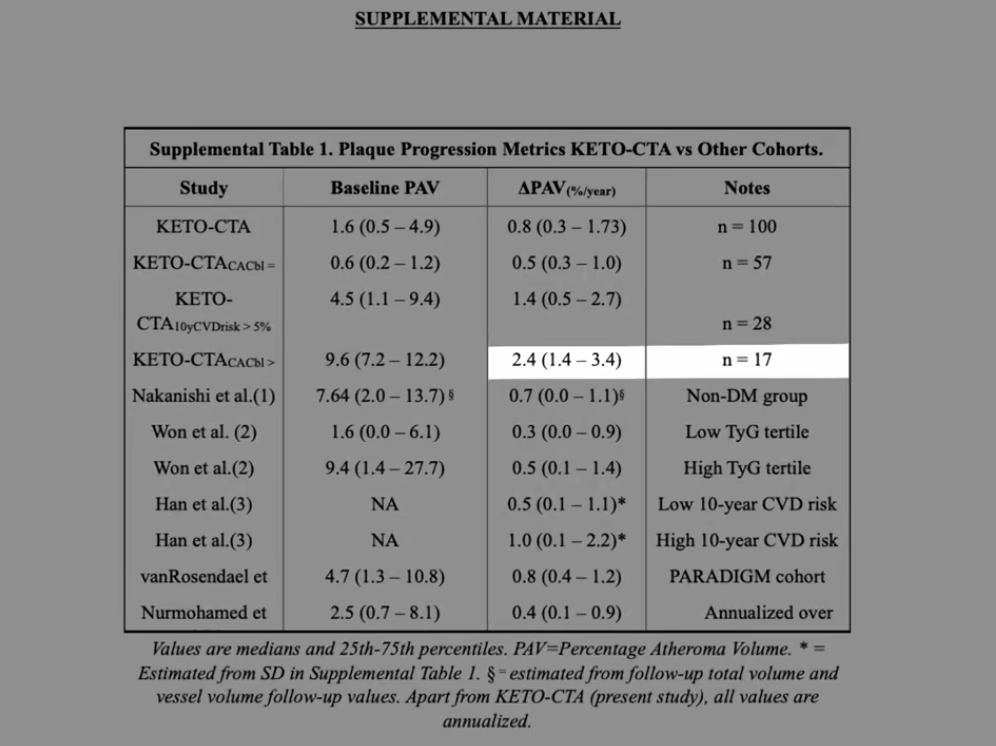
Dr. Budoff: Imagine if I had a patient in my practice and they had a calcium score above 100 and I said, “OK, we’re going to do no interventions and we’re just going to see what happens to your score.” We know what happens. The calcium score goes up a lot and we can look at change in calcium score as well, which we have an incredible amount of data on, showing that some people are very rapid progressors. I think in those patients, we have to look for inflammation. We have to look for tightening blood pressure control. We have to look at other factors. And to be quite honest, irrespective of this group, they came in with a lot of plaque at baseline, meaning likely well before they ever went on the keto diet, they had atherosclerosis that was going untreated. And we need to make sure that we take these patients who have plaque and look for ways of intervening to lower their cardiovascular risk. And we didn’t do that purposefully in this one year trial. But now I’m recommending to many of them that they look more carefully at their cardiovascular risk factors and that they make sure that they’re treating these other factors that were going untreated up until now because they were unrecognized as having plaque. They didn’t know that they had the disease. So they weren’t treating the disease. We identified that with our CT angiogram.
Dr. Scher: Right. And I guess a lot of people want the answer. Well, then what’s causing the plaque, which is kind of an unanswerable question. But based on what we see in this study, can you say that the keto diet itself is contributing to plaque progression?
Dr. Budoff: That’s what we set out to prove. We proved that the keto diet specifically did not cause the plaque progression. We looked at the interaction between the induced LDL and the change in plaque, and we could not find a relationship. So we know it’s not the keto diet causing the plaque progression. We know that plaque begets plaque; that’s been known for a long time and we re-established that. And I would suggest to these patients that despite doing all of this wonderful stuff that they’re doing for their own health with the ketogenic diet, that they look towards going on other therapies that are proven to help with atherosclerosis. And I actually do talk to my keto patients who have a lot of plaque at baseline. I do a CT angiogram on all of my patients who are on the keto diet. And if they have a lot of plaque, I recommend an aspirin tablet at low dose. I recommend tight blood pressure control. And I do recommend a statin for those patients, not to treat the keto-induced LDL, but to treat the underlying plaque that they have, because we know that we can slow down plaque progression regardless of the cause with a statin. Statins work even in low LDLs to lower plaque burden. We’ve studied that extensively. So I do recommend treatment of these patients, but I let them continue the keto diet as long as we can control the other cardiovascular risk factors and make sure that they’re not progressing or remain untreated.
Dr. Scher: Thank you for that clinical insight. I think that’s really helpful. So now lets rewind for a second, you brought up the Miami Heart match which showed in a matched cohort for metabolic health despite drastically different levels of LDL the group on keto with very high LDL did not have higher plaque scores than the Miami Heart. So now it gets a little confusing because we are using different measurements. So it was reported as total plaque score and the coronary score score so tell us how those differ from the PAV.
Dr. Budoff: Total plaque score is a very well adapted tool without quantitative A.I. measurement of the atheroma. So when we read the study, we read each plaque in each segment to see if there is plaque present. Is it mild, moderate or severe? And then we sum up all of the plaque in a semi-quantitative way to get to a total plaque score. It’s been exceptionally well validated. It predicts outcomes. And before we had these A.I. tools, it was the simplest way of looking at all of these metrics. We didn’t have PAV percent measured by Cleerly in the Miami Heart population. So we couldn’t compare plaque volumes in this way. But we could compare total plaque score. We looked at that very carefully. They were all read by my lab, all QA’d by my lab and by me. So very, very reliable measurements. We saw no significant difference between the baseline keto scores and Miami Heart. The keto patients had been on the diet for an average of four years. The amount of plaque they had, versus the Miami Heart population (despite the Miami Heart population having a much lower LDL) were similar. Now, both of them had some plaque and both of them probably deserve some other therapies. But again, this was a population-based study, Miami Heart versus an asymptomatic population, the Keto-CTA trial. And I think it was a very fair comparison to show that they had similar plaque volumes. So, again, another point of proof that it wasn’t the keto diet driving the plaque, but it was other underlying risk factors. Remember, there are probably 50 risk factors for heart disease, diabetes, hypertension, Lp(a), inflammation, etc.. We’re not controlling all of them with any one intervention. Looking at the natural history of plaque and showing that it wasn’t driven by this LDL-induced change on keto is the primary answer. I think we answered that question very definitively.
Dr. Scher: Will there be future papers from this cohort looking at Lp(a) and inflammatory markers and other blood tests and risk factors that you did monitor?
Dr. Budoff: Absolutely. We did extensive blood testing. Dave Feldman actually flew the blood over to the lab personally to make sure it didn’t get lost in transit. We put it on ice and shipped it to make sure that the samples were received and that we have a complete data set. We now have numerous biomarkers that we’re going to look at, including Lp(a). We also have a lot of work to do on non calcified plaque volume. There was some increased there as well as PAV. And we want to look at that and compare that. And also of interest, we now have the Cleerly measurements in the Miami Heart study. So we can now go back and look at the PAV percent in the keto group and the PAV percent in the Miami Heart group and compare the two. We can not only look at total plaque score, we can look for more nuances between the the two groups to further answer this question. So there’s a lot more to come.
I don’t think people should criticize a first paper when clearly there are multiple papers being planned that will lead to multiple answers. And there is nothing hidden here. These tables, if anything, were too explicit. I could tell you that this was a very incomplete list in this supplemental table one, which has received a lot of criticism. But I just presented the EKSTROM trial on Colchisine. In the placebo group, the Delta PAV change was 1.4. In the placebo group! The Delta PAV was 1.4 in one year. That’s very similar to the Keto-CTA group. If you look at the people who had higher risk, and these patients were at higher risk, it was almost identical. And there was no outcry that that’s a large PAV change. And we didn’t calculate PAV percent change percent from baseline change. We didn’t do percent of percent changes because that’s not how we analyze the data. This happened with my EVAPORATE trial. People who are naive to studying plaque progression make the wrong calculations and make a big deal about nothing. I think we just have to ignore the non-scientists and non-clinicians who don’t have a clear understanding. In the medical literature in PubMed, you see mostly scientists addressing scientists, so it’s a civil discussion, and it’s scientifically based. I think we lose that a little bit with Twitter or now known as X.
Dr. Scher: Well, I think the one benefit of the discussion, though, is it’s spurring deeper conversations like this. I mean, the whole world now is hopefully going to learn a lot more about PAV and interpreting PAV, which they didn’t know before. So hopefully that’s a benefit.
Dr. Budoff: I just don’t like the negative context and some of the, dare I say, immature comments that are made. As you know, there’s no reason to get personal. I don’t know these people. And I don’t need personal attacks on my integrity or my science based on somebody who’s never done research, who’s never published a paper. You want to point out a scientific point? Please do. But let’s keep it positive. I mean, let’s engage without casting dispersions that are totally unnecessary. I wish they could ban that kind of banter as well. It’s just not helpful.
Dr. Scher: Yeah, I mean, that’s a very reasonable response for sure. But just to summarize: The placebo group in the EKSTROM trial, which was similar at baseline to the higher-risk Keto-CTA group, also had a 1.4 PAV change in one year. So very similar with no outcry for that. So that is certainly interesting.
Dr. Budoff: And I just want to say the EKSTROM group at baseline were treated with many therapies. That was not a treatment-naive population. They were treated with statins. They were treated with aspirin. They were treated with blood pressure medicines, and they still had a 1.4 percent change in one year. So they had multiple therapies on board and had the same PAV change as the higher risk Keto-CTA patients who had no therapies on board. So again, you know, it’s still apples to oranges, but should be reassuring to everybody that this is not outrageous. And this has not been a novel finding or something that’s never been seen before. This is common, to see plaque progression in high-risk people. And we saw plaque progression. And all we were looking to do was ask: “What caused the plaque progression?” We weren’t trying to say that plaque can’t progress. I didn’t expect that everybody in the keto trial who had plaque would have zero scores, or that the keto diet was liquid Drano that would clear out the coronaries. But I think we established our goals in a very safe and scientific way.
Dr. Scher: Excellent. You brought up the non-calcified plaque volume (NCPV). Tell us how that differs from PAV. Let’s again start from the basics, and then we’ll talk about what changed.
Dr. Budoff: So PAV is total plaque. Very simply, it’s all the plaque: It’s calcified plaque, it’s fibrous plaque, it’s fibro fatty plaque, it’s low attenuation plaque. It’s all the different plaque changes and plaque volumes across the spectrum. Non-calcified plaque volume excludes the calcified plaques. So it’s not all of the plaque volume. It’s only that volume that we deem is soft, if you will. That’s a term we often use, “soft plaque” or “non-calcified plaque.”
Dr. Scher: And that’s because that’s thought to be higher risk plaque? So is that the reason for focusing on it?
Dr. Budoff: We think it’s more amenable to change. Sometimes calcified plaque doesn’t change much and rarely, if ever, can go down. So we look at a non- calcified plaque as a perhaps more modifiable plaque for a target for treatments. For example, if we were putting somebody on an intervention, we would look for non-calcified plaque, often as a primary, to see what changes because the calcified plaque doesn’t change as much.
Dr. Scher: Right. So does it tend to go in step then with PAV as PAV changes, non-calcified plaque changes, sort of in general, kind of loosely correlated?
Dr. Budoff: Yes. Unless something specifically causes a high calcification rate, they should be very parallel. Because there’s so much outcome data with PAV and PAV percent changes, we wanted to focus on that as an end-point. The non-calcified plaque volume went up similarly; it went up in parallel. We’re going to have a whole separate paper coming out that’s going to delve into some of these other plaque volumes that we looked at in the keto trial. Fibrofatty plaque, non-calcified plaque, fibrous plaque, low attenuation plaque, and total non-calcified plaque as well. But we couldn’t put everything in the first paper. And it certainly wasn’t being hidden, as some people suggested, because it was in the supplemental material or is in the table itself in the paper. So, you know, we were forthcoming, but we couldn’t focus on everything in this first paper. And we certainly are going to look at that change in non-calcified plaque volume in much more detail and compare that to the baseline non-calcified plaque volume to the Miami Heart population as well. So we’ll have a more quantitative look, as I mentioned earlier.
Dr. Scher: Oh, that’s great. I really look forward to that. Because if you look at figure one in the paper, it does list the delta non-calcified plaque volume. And, you know, for people who aren’t used to looking at this, it’s listed for each individual. Some are going to have steeper lines; one person has a very steep line, other people have very shallow lines. I guess it’s hard to know exactly how to interpret that, but what’s your take on that change? And then I guess it’s couched with the comment that more is coming with future papers as well.
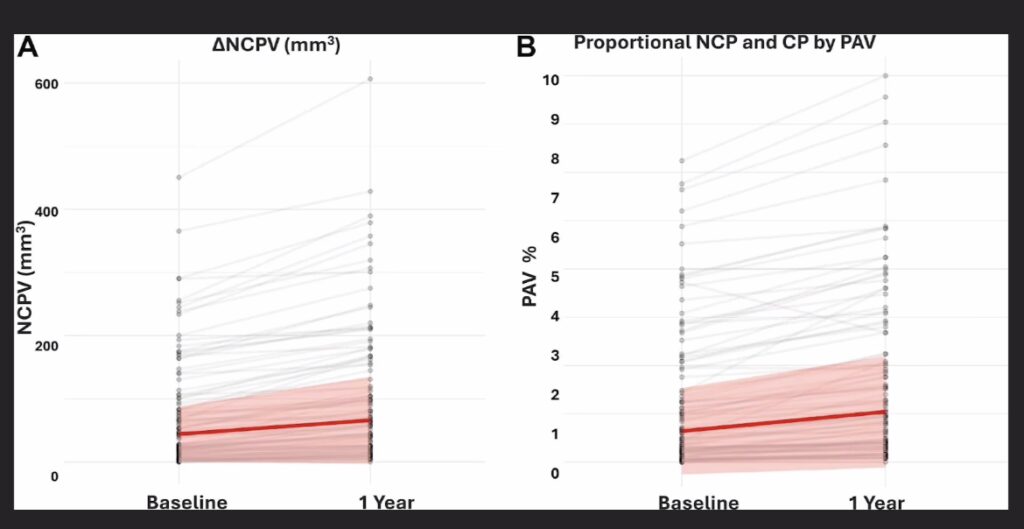
Dr. Budoff: I think the purpose of figure one, which I thought personally was very clear, is that in the Figure A, the change in non-calcified plaque volume was identical to the PAV, which was on the right. That was the reason for putting it in the paper — to show that it’s identical. If anything, the PAV was a slightly steeper curve upward. So you could argue that we put our worst foot forward if we were trying to do anything here by couching this in PAV, instead of non-calcified plaque volume, because at least visually, the slope looks steeper in PAV. And that’s what we reported as our endpoint. But again, we chose PAV because we have so much data with PAV from so many other interventional studies, and we don’t have the same with non-calcified plaque volume; we just don’t have that same wealth of data. But we will be presenting that as well. If anything, people should be reassured that non-calcified plaque volume is similar or better than PAV. So, what we presented for PAV should be encompassing non-calcified plaque volume.
Dr. Scher: Well, I think this has been a wonderful tutorial on just these measurements by themselves, but then also how it relates to this paper, and the interpretation of the paper and, safe to say that we can’t say keto protected everybody from plaque, and we can’t say keto made everybody worse. It does appear that the plaque change was not associated with LDL, but that doesn’t answer questions as to what it is associated with. And there are many future papers to come, looking both at this and the non-calcified plaque volume, other risk factors, and higher lower-risk groups within this Lean Mass Hyper-Responder phenotype. So there’s much more to come. And I appreciate you very much giving us this very reasonable explanation about all this. So any other last words to sum up?
Dr. Budoff: I would just say: I welcome comments, criticisms, and other thoughts. Just please, let’s just keep it civil and have civil discussions. And I’m glad to engage people in more healthy debate about what we found, and what it implies, and what it means and what we should do for our patients who are on the keto diet who do have this induced LDL change.
Dr. Scher: That’s a good point I would like to finish with: This has real world implications, right? We’re talking about this because we want to help these individuals and nobody else has studied this. That’s the thing we also have to put in perspective. This discussion would never have happened without this study. When I see these patients in clinic, they’re constantly asking if there is any evidence about what to do? And now we’re starting to get evidence and there’s much more to come. But none of this would have ever happened without your efforts and the efforts of your team. That deserves recognition. So thank you for that.
Dr. Budoff: Thank you. That’s why I took the study in the first place. I had no stake in the game. I had no preconceived notions about what we would find. I took the study because I thought it would not only answer an important question, but hopefully lead to better treatment for patients who are benefiting from the keto diet, who are seeing an induced LDL change, and what we can do about it, and what the implications are of it. I think we’re going to learn more, but I applaud all of those people who crowdfunded this study, who were able to make this happen and put in a huge amount of effort to get this published and to get this out into the community. I hope we can continue to engage in civil dialogue and learn from it. We’re going to continue to publish more papers, and hopefully inform people about the true implications for our coronary arteries.
Dr. Scher: I hope this interview was helpful. I sure got a lot out of it. And I really think we have a better understanding of what these measurements are. And I guess the drawbacks of trying to ask too much of one publication and one study. Fortunately, there are many more to come. We also have a lot of other material about this study. So if you’re interested in some of our other interviews, both with Dr. Budoff and with Dave Feldman, and then a video I did myself, they will be listed in the description below with any other material that comes up in the meantime. So I hope this was helpful.
The science is not settled. We will continue to learn more, but I think we’ve learned a lot up to this point.