How can a metabolic intervention succeed where potent, “evidence-based” pharmaceuticals have failed? In this compelling guest post, originally published on his ‘StayCurious Metabolism’ newsletter, Dr. Nicholas Norwitz challenges the conventional boundaries of psychiatry. He makes a powerful case that many severe mental illnesses are rooted in metabolic dysfunction, and offers a clear and compelling look at the future of mental health treatment. You can subscribe to his Substack here.
“Is metabolic psychiatry a real science?” It’s a question at the heart of an emerging field you’ll be hearing a lot more about in the coming years, one that will fundamentally change our approach to mental health — for the better.
But let’s start by painting a picture: Imagine a patient suffering from a severe mental illness (SMI)—perhaps schizophrenia, bipolar disorder, major depressive disorder, or obsessive-compulsive disorder.
They’ve tried multiple pharmaceutical interventions, yet nothing has worked. These are individuals with drug-refractory SMI in whom even the most powerful neuropsychiatric medications have failed.
So, the idea that metabolic health interventions—often grounded in nutrition—might offer relief sounds fantastical. How could fasting and a plate of salmon, avocado, and eggs succeed where potent “evidence-based” pharmacology has failed?
I understand the skepticism. But let’s take a closer look.
Here’s the path we’ll take in this letter:
- First, we’ll break down the limits of our current “evidence-based” medicine and why it often falls short in treating chronic mental illness.
- Then, we’ll dive into three recent studies that provide concrete, biological proof of the link between metabolism and mental health.
- After seeing the science, I’m going to share with you four powerful stories directly from patients, or their care providers, who reversed “untreatable” conditions like schizophrenia and bipolar disorder using dietary interventions.
- Finally, we’ll look forward and discuss why the future of psychiatry must have a metabolic lens.
Why We Trust Pills: The Gold Standard and Its Limits
Contemporary Western medicine is built on a specific hierarchy of evidence, with the double-blind, randomized controlled trial (RCT) regarded as the “gold standard.”
In these studies, participants are randomly assigned to receive either an intervention—typically a drug—or a placebo, without knowing which group they’re in. This design helps eliminate bias, including the placebo effect, and aims to isolate the true impact of the treatment. It’s through this rigorous methodology that we define what qualifies as “evidence-based” and what becomes the standard of care.
There are several inherent problems with the current model of “evidence-based” medicine.
1. One Size Doesn’t Fit All
First, clinical trials necessarily recruit heterogeneous populations—after all, human beings are not all the same. As a result, the outcomes observed in group averages may not accurately reflect how an intervention will affect any given individual. It’s entirely possible for a study to yield statistically significant results, receive publication in a top journal, and lead to the release of a blockbuster drug—while that drug benefits only a small fraction of patients.
In fact, among the top ten best-selling drugs, most help only between 1 in 4 and 1 in 25 people who take them.
2. If There’s No Profit, There’s No Proof
The second issue is economic: the biomedical research system is not well-suited to study interventions that lack a clear commercial incentive. For example, testing the effects of dietary interventions on mental health is far more difficult than testing the effects of a pill. Diet studies are hard to blind or control with placebos, and extremely expensive to carry out. That’s not even to mention recruitment and compliance issues. Simply put, the obstacles to conducting these studies are greater and the rewards —financially speaking— minuscule. Once the study is complete, the paper written, and the article processing fee paid, who profits from a dietary recommendation?
This isn’t to vilify the pharmaceutical industry. But we must be clear-eyed about what “evidence-based” medicine actually means, or does not mean, within the confines of the system we’ve built.
3. Treating Symptoms, Not Causes
Third—and arguably most important—conventional evidence-based medicine often fails to address the root causes of mental health disorders. The current system for developing treatments is, in many ways, remarkably crude. It’s like trying to fish blindfolded by firing a pistol into opaque water—random, imprecise, and largely guesswork. In practice, we throw pills and procedures at the problem and hold on to whatever seems to stick.
Historically, this trial-and-error approach has been necessary. The brain is notoriously difficult to study in living humans. Metabolically, it remains a black box—an unfathomably complex organ producing the emergent phenomenon we call the mind. We’re dealing with three pounds of soft tissue, housing nearly 90 billion neurons and trillions of constantly shifting synaptic connections. Trying to untangle this with scientific precision feels almost impossible. “Intimidating” doesn’t even begin to capture it.
Everything you’ve read so far is meant to explain how we arrived at our current state—and why it makes sense that people are skeptical of the idea that food, sleep, exercise, and metabolic health could play a central role in treating severe mental illness.
But I’m here to tell you: Metabolic Health is a necessary part of the solution to the Mental Health Epidemic.
Why?
Because at its core, the brain is an organ like any other. And like all organs, it becomes vulnerable to chronic disease when the foundational systems of metabolism begin to fail. These failures include pathological processes such as oxidative stress, inflammation, and mitochondrial dysfunction. I understand these terms might feel abstract—jargon, even—for those without a scientific background.
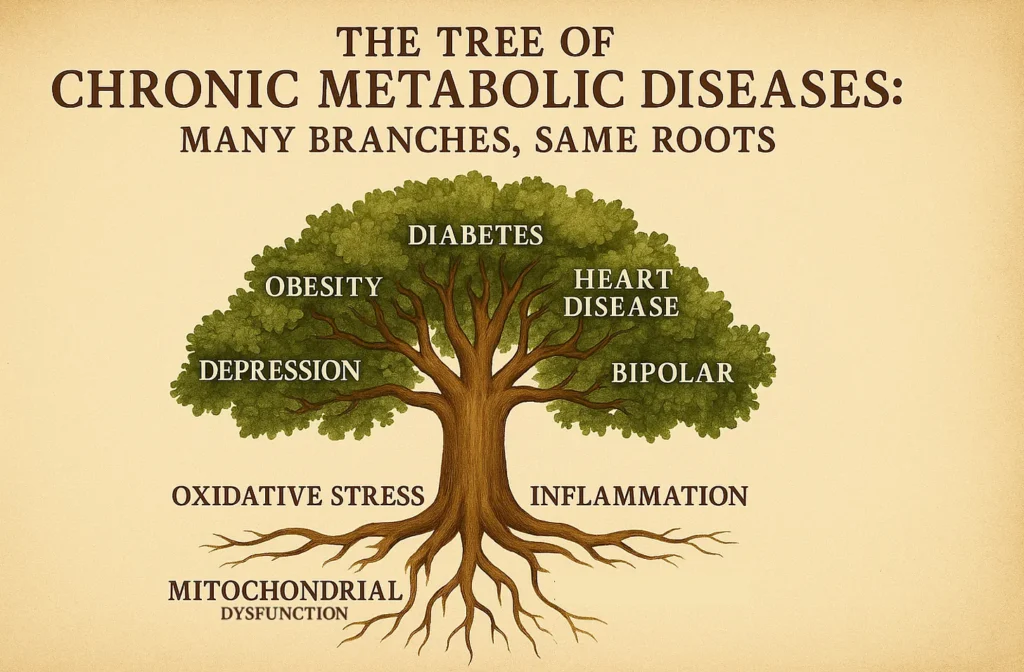
The Tree of Chronic Metabolic Diseases: Many Branches, Same Roots
So let me offer an analogy: these metabolic disturbances are like the roots of a tree. From these roots grow the entire tree of chronic metabolic diseases—obesity, heart disease, neurodegenerative conditions, diabetes, and yes, even severe mental illnesses.
That’s not to discount the psychological or social factors that contribute to mental illness—far from it. But even those forces ultimately converge on the health of our metabolism.
Inflammation and Anxiety: A Direct Biological Link
Chronic inflammation can be measured by biomarkers—specifically, elevated levels of signaling proteins called cytokines circulating throughout the body. In a 2025 study published in Cell, researchers identified a striking finding: one such molecule, the inflammatory cytokine IL-17, doesn’t just trigger immune responses in the body—it also acts in the brain as a neurotransmitter that amplifies anxiety. When neurons receptive to IL-17 are activated, anxiety increases; when they’re dampened, anxiety decreases.
This is more than a correlation. It’s a clear, causal link between inflammation—a core metabolic dysfunction—and a mood disorder that affects millions. Anxiety, in this case, isn’t just psychological. It’s biochemical.
Autophagy and Despair: Cellular Dysfunction in Depression
Autophagy is a fundamental cellular process—the body’s way of cleaning out damaged components and recycling them for optimal function. It’s essential for metabolic health at the cellular level. And new research published in Nature (2025) suggests that impaired autophagy may be a root metabolic cause of depression.
Here’s how it works: chronic stress, a major trigger for depression, can suppress autophagy in a key brain region involved in mood regulation—the lateral habenula. When autophagy slows down in this area, cellular debris builds up, including receptors for glutamate, the brain’s primary excitatory neurotransmitter.
The result? An intensified glutamate (excitatory) signal in the very center of the depression center of the brain. The consequence is not abstract—it’s a neurobiological intensification of despair.
What’s particularly interesting is that multiple classes of antidepressants, including SSRIs and ketamine, appear to target can converge upon this very dysfunction. They restore proper autophagy in the lateral habenula, which may be one of their key mechanisms of action—suggesting that improving cellular metabolism isn’t just incidental, but central to healing.
For more, click HERE for the full letter and HERE for the video breakdown.
A Probiotic for Depression? Hope in Homovanillic Acid
There are metabolic signatures of mental health disorders—one example being idiosyncrasies in the microbiome that track with depression. A study published in Cell Metabolism (2024) found that patients with depression have lower circulating levels of a hormone and neurotransmitter called homovanillic acid (HVA), a metabolic cousin of dopamine. These patients also had reduced levels of gut bacteria that support HVA production.
There’s reason to believe this is not just a correlation, but a causal relationship. First, unlike serotonin produced in the gut, HVA can cross the blood-brain barrier. Second, the researchers conducted experiments in multiple mouse models of depression and found that supplementation with HVA—or with bacteria that produce HVA—was sufficient to improve depressive symptoms across several behavioral tests.
The data are still early, but extremely hopeful.
- For more, stay tuned. I’ll be releasing a full letter dedicated to this study in the coming weeks.
I could easily continue with more examples—even were I restricted to reporting only on findings published this year in highly reputable journals. But by now, I think the core message is clear. And this leads us to a crucial point: the real-world impact of recognizing that many mental health disorders are, at their root, metabolic in nature.
From Theory to Practice: What Happens in Real Patients
The true power of this insight emerges when we translate it into clinical practice—when we apply nutritional and metabolic interventions to patients suffering from severe, treatment-resistant mental illness. The results are not theoretical; they’re visible in the lives of real people.
But don’t just take my word for it. What follows are the voices of patients themselves, drawn primarily from recent case series across a range of serious psychiatric conditions. I’ve included the original sources for those who want to explore the primary research firsthand.
Patient, Obsessive-Compulsive Disorder
I used to tell myself in the depths of OCD, ‘The only way out is death,’ as a kind of mantra to put things into perspective. I’m happy to say I found another way. It would make me really happy if others knew about ketosis as a way to end their suffering.
My son has seen me through a lot. I remember when I was at my worst on a feeding tube and too weak to walk, he used to sit by my bed and stick the hose from his toy firetruck up his nose to mimic his mommy. Now, I’m looking forward to bringing him to a trampoline park for his eleventh birthday and jumping alongside him! A ketogenic carnivore diet cured me – mind and body. Eating this way gives a calmness and clarity of mind I can’t even describe. I’m so grateful to be here today and wanted to share my story because I know there are others out there like me who can benefit from this lifestyle.
Mother about her Son, Bipolar Disorder
Matt stayed on his medications and did everything he could to get well. He was treated by 41 clinicians and prescribed 29 meds before his psychiatrist pronounced his illness treatment resistant… after nearly five years of battling bipolar illness, Matt started a ketogenic diet… [by] that spring, Matt needed only quarter of the dose of medication he’d needed the year before to fend off mania. Within four months, his mood was stable, and his intellectual vitality had returned. He graduated from college and now works full-time in tech…”
Physician about his Patient, Schizophrenia
Patient A is an 82-year-old female diagnosed with schizophrenia since the age of seventeen. Her symptoms included chronic paranoia, disorganized speech, and both visual and auditory hallucinations – seeing skeletons and hearing voices on a daily basis. She had numerous hospitalizations throughout her life for psychosis and suicide attempts… Within two weeks [of starting a ketogenic diet], she noted a marked reduction in her psychotic symptoms…She [now] takes no medications and remains free of psychotic symptoms, and has also regained her independence, no longer requiring the care of a PACT team and no longer having a guardian. She lives independently and reports that she is happy to be alive.
The Future of Psychiatry Demands a Metabolic Lens
We are witnessing the early days of a transformation—one that demands we rethink what mental illness is, how it arises, and how it can be treated.
The stories you’ve just read are not isolated miracles—they’re not even miracles at all. They are proof-of-principle.
When we address the foundational metabolic dysfunctions driving the brain into chaos—when we nourish it, stabilize it, and give it what it needs to function—healing becomes possible, even in the most severe and “untreatable” cases.
This isn’t speculation. It’s not fringe theory. It’s emerging science, grounded in physiology and clinical reality. And it demands our attention. If metabolic psychiatry challenges the old model, it’s only because the old model left far too many behind—patients who were told they were “treatment-resistant,” when in fact, they were metabolically unwell.
It’s time to evolve the conversation. To recognize that the brain is not a separate, ethereal entity—it is tissue, powered by mitochondria, damaged by inflammation, healed through food, movement, sleep, and biochemical balance.
Metabolic psychiatry does not reject the tools of conventional medicine—but it expands the toolkit. It reintroduces common sense, clinical observation, and biochemical integrity into a field that has long been dominated by blind pharmacology.
This is not the end of the story. It is the beginning of a new chapter in mental health—one rooted not only in data and molecules, but in hope.
The future of psychiatry will be metabolic. And for many patients, it can’t come soon enough.
About the Author
Dr. Nicholas Norwitz is a leading voice in the science of metabolic health. He earned his PhD at Oxford and MD at Harvard, and his work aims to make metabolic health science accessible, bridging the gap between rigorous academic research and practical health solutions. You can read more of his work by subscribing to his newsletter, ‘StayCurious Metabolism.’